Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
25-NOVEMBER-2014 ALAA ABDEL-SATTAR HAMDI 51 YEARS
CYSTIC INTRAMEDULLARY LESION OF THE CONUS MEDULLARIS BEHIND L1.
Anamnesis
The patient came to the clinic 22-November-2014
complaining of LBP for 50 days without sciatica.
Difficult walking that she cannot walk more than
300 meters, after what getting left hip pain.
The condition of the patient is deteriorating.
On examination, the patient is limping with
exaggerated scoliotic stance. SLRS 70 degrees
both sides with weak both lower limbs 4/5 both
sides.
The patient was sent for MRI of the dorsal and
lumbar spine with contrast and single voxel
spectroscopy. There is a cystic intramedullary
lesion inside the conus medullaris and it is
stuck to the posterior wall of the dura. The
content of the cyst is CSF like consistency and
spectroscopy ruled out malignant changes of the
lesion.
Using the C-arm, laminectomy of L1 was
performed. The dura was opened longitudinally,
trying during that to preserve the adherent to
it the underlying arachnoid which was separated
from the dura by sharp dissection. It was
necessary to dissect the arachnoid
circumferentially to remove the arachnoid cyst
and part of it was sent for histologic
verification and after its removal the spinal
cord was hanging free. Using Inomed with DNS
revealed no response even with 10 mA and it was
assumed that the ISIS Inomed was
troubleshooting. The dura was closed
water-tightly and routine closure of the wound.
Before weaning off the patient, she was sent for
MRI investigation, which confirmed the still
presenting intramedullary cyst. The wound was
opened and a 3 mm incision over the
nonfunctioning part of the spinal cord was
performed. The fluid was sent for histologic
verification and the spinal cord collapsed
completely and running nearby roots were seen.
The roots were responding well even with DNS
below 2 mA both sides. Routine closure of the
wound.
Smooth postoperative recovery. The
power of both lower limbs normalized.
Comments
When you have suspicion, always check.
The no response of the spinal cord to DNS at the end of
first stage of surgery led to perform intraoperative MRI
which confirmed the still persisting intramedullary cyst.
The pathologic non-functioning posterior spinal cord was
opened to evacuate the cystic cavity, after what the
functioning neural tissues came to the field.
It is rare to see syringomeyletic cavity
at the conus medullaris level. This was mostly triggered by
the presenting arachnoidal adhesions of this area to the
dural wall.
Even with the best MRI available
technology, a misleading data can lead the neurosurgeon to
wrong conclusions. All the time check when you suspect.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
Inomed MER system
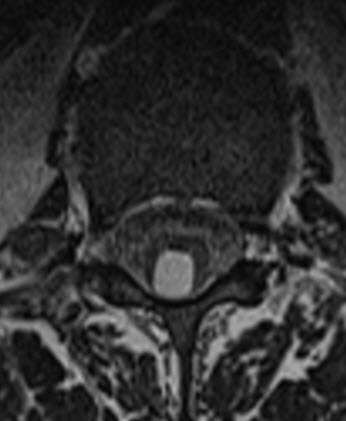
Axial T1 weighted MRI showing the cystic lesion adherent to the
dura.
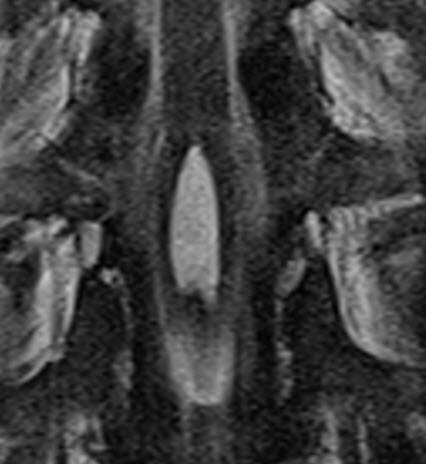
Coronal T2 weighted MRI showing the cystic lesion inside the conus
medullaris.
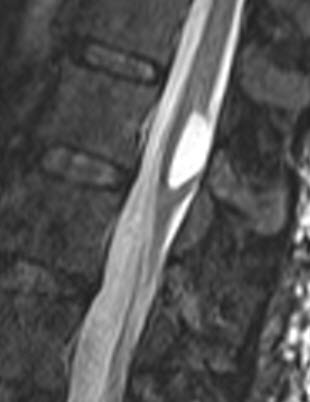
Sagittal T2 weighted MRI showing the lesion.
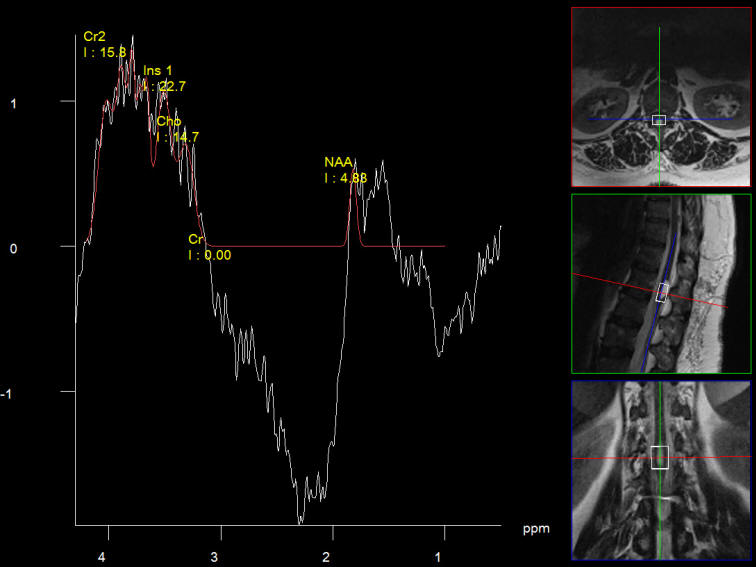
Single voxel spectroscopy ruling out any malignant nature of the
lesion.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .