Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
15-JANUARY-2015 ALI HASAN AL-RAS 46 YEARS COMPLETE STENOSIS
OF THE RIGHT ICA WITH RECURRENT STROKES.
Anamnesis
The patient came to the clinic 27-February-2011
complaining of weak left upper limb with feeling
of cold of this limb for 9 months. MRI cervical
spine done 27-May-2010 showing bulge disc C4-5.
ECS done 26-December-2010 reporting
demyelinating neuropathy both upper limbs. On
examination at that time; the Romberg position
was stable, but the left upper limb swaying
down. There is hypalgesia of the left side of
the face and the left upper limb with weak
muscles left upper limb 3/5, except the left
deltoid muscle. The patient was sent for
investigations and MRI of the brain done
02-March-2011 showing malacia of the right
parietal lobe with complete occlusion of the
right ICA 10 mm above the bifurcation of the
right CCA. MRI cervical spine showing the same
data as before. Cardio consultation was
uneventful. The patient underwent carotid
angiography elsewhere and attempt to perform
stenting 30-January-2012 failed. MRI of the
brain with MRA repeated 31-December-2012 showed
still complete occlusion of the right ICA. The
patient 09-May-2013 was advised to undergo
endarterectomy, but he escaped. The patient then
came 25-December-2014 telling that he got
another attack of infarction, and he was told
that it was in another territory?
On examination, the patient is alert with the
weak left hand extension and flexion -3/5 and
weak dorsiflexion left foot.
The patient was sent for investigations and MRI
of the brain and done 28-December-2014 showing
the same data as before. He was another time
advised to explore the right ICA territory.
Exposure of the right CCA, ECA with the branches
arising from the last. The right hypoglossal
nerve was dissected and preserved. There was a
huge lymphnode in the area which was resected to
obtain visual control in the field. The ICA was
followed from distal to proximal to be sure that
no abnormality could be present at the
bifurcation. The right ICA is hypoplastic and
its external diameter less than 3 mm. Direct
angiography done demonstrating that the ICA is
completely occluded 10 mm above the bifurcation
and no pulsation is noted. After clamping of the
right CCA and ECA arteriotomy was done. There
was an atheroma completely occluding the right
ICA. It was removed but no back flow was
obtained. Using subclavian catheter No 20 three
way with the brown canula connected to the end
of the catheter, gradual dilatation and cleaning
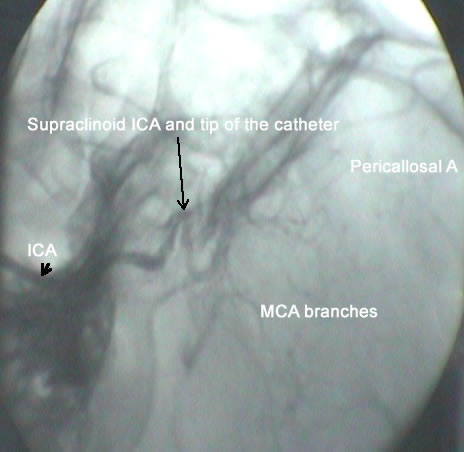
with saline and heparin was applied. Using the
C-arm, the tip of the catheter was followed and
continuous angiography and cleaning was
performed until the right ophthalmic artery was
seen. The segment above this level up to the
bifurcation of ICA to A1 and M1 which usually
3-5 mm in length required 20 min and 10 passes
to clean and dilate the area until proper
angiography of the right circulation was
established. The canula was removed and there
was back flow from the ICA. Using Dacron patch
the arteriotomy site was closed and control
hemostasis was achieved after removing the
clamps. The hypoplastic ICA regained good
pulsation after that. Routine closure.
Smooth postoperative recovery.
The power of the left upper limb became normal.
Comments
The patient underwent angiography
elsewhere and attempt to introduce a stent failed.
The findings during surgery explain the
cause of this failure. The hypoplastic right ICA not only
completely occluded, but it became hypoplastic over the
years. The subclavian canula with great difficulty could
pass the artery lumen.
If the dilatation of the hypoplastic
artery did not succeed and the angiography of the right A M
was no seen and the back flow did not appear at the end of
the procedure, than it was planned to make bypass from the
CCA up to the supraclinoid part of the right ICA.
Of course the artery now is hypoplastic
but it could dilate with time or return to the preoperative
status. Time will tell the result.
Heparin was not used during surgery,
because the flow to the right ICA was 0% and the artery was
continuously dilated and irrigated all the time until back
flow was seen. Aspirin was not topped preoperatively and
Clexane 40 mg was administered 12 hours after surgery.
The cause of hypoplastic artery is the
complete occlusion and long period of time elapsed since the
occlusion with absent flow in the involved segment.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
Inomed MER system
The circulation restored after long effort.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .