Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
06-OCTOBER-2012 AMAL MUHAMED ALFAQIR 48 YEARS
FAILED NECK SYNDROME AFTER SEVERAL SURGERIES.
Anamnesis
The patient came 20-August-2005 complaining of
severe neck pain with bilateral radicular
syndrome for more than 15 years. Exacerbation
for the last 4-5 months with inability to rotate
the head for all directions and fainting attacks
with weak grip, extension and triceps both upper
limbs with hypalgesia of the left C4 and 5
dermatomes. The patient was operated
24-August-2005 and discectomy of the C4-5 disc
done, where a fresh fragment came from a defect
in the PLL after applying traction and the C5-6
was old, requiring drilling with
osteophytectomy. Syntex cervical miniplate with
6 screws 14 mm length were applied to fuse the
C4-5-6 with traction of 12 Kg applied during
that.
The patient showed dramatic improvement of her
neurological deficit, but she came
15-October-2005 claiming of left sided
hemihyplagesia without motor deficit. Migraine
was considered as the cause of her complains and
she was sent for MRI of the brain and MRA of the
brain and carotids, which proved to be normal.
The patient escaped and reappeared
27-October-2006 after undergoing elsewhere, left
CT release and an incision in the posterior
aspect of the cervical spine with severe atrophy
of the the paraspinal muscles left side with
agonizing pain, that it was impossible to touch
her left upper limb. No documents available
explaining what was done in the posterior
cervical spine. Sympathetically mediated pain
was suspected.
All the time check MRI of the cervical spine was
performed, confirming that the construct is in
place and no compression was noted.
The patient came 28-August-2007 with severe
bilateral radicular pain more severe in the left
side with frozen shoulder both sides . She felt
down 06-May-2007 with fracture right foot and
underwent hysterectomy 18-August-2007. SLRS was
20 degrees both sides and she was sent for MRI
lumbar spine and dynamic study for the cervical
spine was requested 01-September-2007.
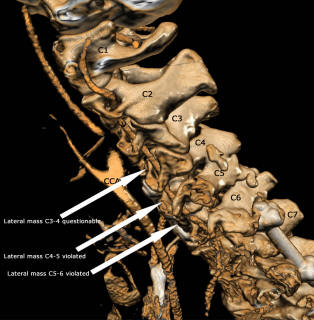
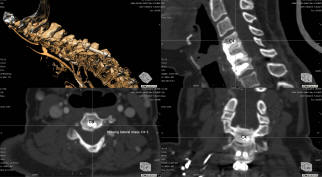
MRI lumbar spine showed bulge disc L4-5. X-rays
of the cervical spine showed missing lateral
masses of the left C4-5 and C5-6.
It became clear that the next surgery was wide
foraminotomy for left C5 and C6 roots without
leaving any bony elements to preserve stability
of the cervical spine.
Several times a detailed discussion was
performed with her and her husband, that the
patient has multiple problems and the only
surgical interventions, which could be suggested
is posterior fusion for the posterior
instability of the spine and left sided
sympathectomy for the sympathetically mediated
pain.
Both agreed and understood the situation and
they were willing to proceed with surgical
treatment.
The surgery was performed 18-October-2007 in the
supine position, under the electrophysiological
control using ISIS Highline Inomed SEP - EMG
protocol.
Skeletonization of C3 down to D3 was performed.
It was noticed that overmobility of the cervical
spine was maximal at C7-D1 and C4-5 levels. The
lateral masses of left C4-5 and C5-6 were
missing.
Sympathectomy of left upper dorsal D2 and D3 was
performed. Both ganglia with their rami albicans
and greysii were removed in one block and the
satellite rami were also coagulated and
bisected.
Using OA System Stryker lateral mass screws 12
mm length, under image-guided intensifier the
normally looking C3-4 both sides masses were
used for upper fixation. The C6 lateral masses
were also used for insertion the middle row. The
infer row was the insertion of 18 mm length
transpedicular screws to the body of D1. Using
rods and bridge the posterior fusion was
achieved after performing slight distraction of
the left rod to resolve possible collapse and
compression of the nerves in the left side.
Routine closure with smooth postoperative
recovery.
The patient came to the clinic 05-February-2008
still complaining of agonizing neck pain and
unable to move her left upper limb. CT-scan
performed 05-December-2007 showing good
alignment of the four lower screws, but with
partial slipping of the upper two screws. She
was advised to keep in medications and protelose
to accelerate the bony fusion.
The patient was advised to be seen after 4-5
months.
MRI lumbar spine performed 22-April-2008 showed
good alignment of the spinal cord and the bony
structures, but did not gave information about
the position of the posterior fusion screws.
The patient then came 17-May-2008 and there was
some improvement of her condition, but
limitation of the neck movements and the feeling
that the upper screws are pushing the upper
cervical spine anteriorly, causing massive
muscle spasm.
The patient was sent for CT-scan of the cervical
spine and simple cervical X-rays, which
confirmed further slipping of the upper screws.
Considering that, a sufficient time elapsed
since the last surgery, and the necessity of the
upper screws is null and in contrary, they are
causing such muscle spasm and limitation of neck
movement, the patient was advised to undergo
partial removal of the upper third of the
construct.
In the laminectomy position, 24-May 2008,
posterior approach was refreshed and the rods
were exposed, just above the level of the middle
screws. The connecting bridge was removed.
Drilling of the rods was performed, as
demonstrated in the postoperative pictures. The
flail screws were removed together with rods.
Routine closure of the wound with smooth
postoperative recovery.
The patient showed dramatic improvement after
the surgery, that myself could not believe in
that. With gradual decrease of pain killers.
The patient came to the clinic 29-July-2009
complaining increased pain in the left shoulder
with limitation of neck movement. She underwent
several surgeries for her cervical spine with
anterior and posterior fixation.
The patient was advised to repeat cervical
X-rays of the spine and CT-scan of the cervical
spine with 3D reconstruction.
The devices were in place and no convincing data
were to be suggested surgically, for what block
of the left C6-7-8 was suggested.
Under G.A. with the use of image-intensifier the
left lateral mass of C5 was reached and using
marcain 0.25% with Diprofos was injected there
and 1cm away. The second target was the left
lateral mass of C7 and the third was the lower
left screw 1 cm lateral to it. The total volume
was 2 vials of Diprofos and 40 ml of marcain.
Upon weaning of the patient, she progressed
respiratory failure, for what reintubation was
performed and waiting for 60 min until she
became alert and acceptable respiratory drive.
The paresis of the left upper limb persisted for
5-6 hours with pain free in the left shoulder.
The patient then came several times complaining
of agonizing pain of the left shoulder and
several investigations were performed and the
only non-destructive solution - spinal cord
stimulation to the C3-5 levels was suggested.
For more information about the suggested
procedure please visit:
https://www.functionalneurosurgery.net/spinalcordstimulation.htm
The patient then came 16-July-2011 complaining
of the same agonizing left upper limb and the
only solution was suggested to undergo insertion
of neurostimulator implant device to the C3-5
level, since no other destructive options remain
in the recent status of neurosurgery.
The patient was reevaluated 16-January-2012 and
CT-scan with MRI of the cervicodorsal spine was
performed 18-Jaunary-2012 which ruled out the
presence of any loosening of the fixating
devices. Now she is receiving Lyrica 150 mg
twice daily, Nexium 40 mg once daily for long
time.
The patient against my personal advice underwent
surgical removal of the posterior fusion in
Bahrain after what her condition deteriorated
more.
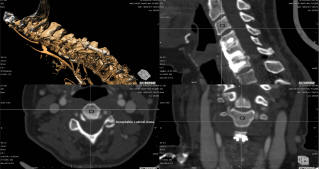
MRI of the cervical spine done 26-June-2012
showing mild concavity at C5-6. CT-scan showed
absent lateral masses at left C4-5, C5-6 and
C6-7 with questionable status of C3-4.
On examination, the patient dramatically
deteriorated after removal of the posterior
fixation. After long evaluation and studying the
case it was decided to stabilize the whole area
anteriorly.
The old anterior incision was
refreshed and exposure and removal of the Syntex
plate was achieved. Discectomy of C3-4 and C6-7
was done. A Scientex Alphatec Spine cage 17x15x5
mm was inserted to the C3-4 level. Another cage
17x15x7 mm cage was inserted to C6-7 level.
Trestle cervical plate 4 level 69 mm length was
used to fuse the C3-4-5-6-7 levels. 4 screws
4.5x14 mm were used for C3 and C4. 4 screws
4.0x14 mm were used for C5 and C7 bodies. All
stages of surgery were done with C-arm control.
Routine closure of the wound. Smooth
postoperative recovery.
Please! wait for 3-5 min till the
video start to load. It depends upon the internet
connection.
Comments
The patient underwent
several surgeries and the main complain is due
to instability of C3-4 and C6-7 in the left
side. Doing surgery from behind was estimated to
be the less optimal solution. Anterior fusion of
C3-7 is the best option to eliminate micromotion
in the lateral masses of the involved segments.
There is problem with most medical companies,
that they are lacking support for their old
versions. When trying to remove an old Zimmer
product, the new screw driver will not be able
to remove the old implant. So the Syntex
Alphatec Spine as happened in this case. The
companies and their dealers must take this
problem into consideration and not to put the
surgeon in a miserable condition, trying to
resolve his problem by his own means.
Conclusion
The patient underwent
several surgeries and the major problem was
after the second surgery performed elsewhere.
The surgeon refused to tell the patient what he
did, but after several investigations it seems
the he drilled out most of the C6-7, C5-6, C4-5
left lateral mass and to lesser degree of the
C3-4. This kind of surgery is missing in the
medical archives and it triggered disaster to
the patient and confusion to the surgeons.
Trying to fuse the segments from behind gave
only partial improvement. Removing the fusion
device in the last surgery triggered the
problem.
During this surgery after removal of the old
construct, it became clear that the C4-5-6
bodies were calcified in one piece. This gave
the conclusion that the major pain generator was
the C6-7 totally eaten lateral mass and
C3-4 both in the left side. Fusing of C3 down to
C7 gave a dramatic improvement of the patient
and she no more complaining of her agonizing
pain in her left upper limb.
This case is rare and to reach to the ideal
solution required a lot of reinvestigations and
surgeries to reach.
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .