 | |
 | |
Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv |
|
Functional Neurosurgery
functionalneuro.surgery
Functionalneurosurgery.net
IOM Sites
iomonitoring.org
operativemonitoring.com
Neurosurgical Sites
neurosurgery.art
neurosurgery.me
neurosurgery.mx
skullbase.surgery
Neurosurgical Encyclopedia
neurosurgicalencyclopedia.org
Neurooncological Sites
acousticschwannoma.com
craniopharyngiomas.com
ependymomas.com
gliomas.info
gliomas.uk
meningiomas.org
neurooncology.me
pinealomas.com
pituitaryadenomas.com
Neuroanatomical Sites
humanneuroanatomy.com
microneuroanatomy.com
Neuroanesthesia Sites
neuro-anesthessia.org
Neurobiological Sites
humanneurobiology.com
Neurohistopathological
neurorhistopathology.com
Neuro ICU Site
neuroicu.info
Neuroophthalmological
neuroophthalmology.org
Neurophysiological Sites
humanneurophysiology.com
Neuroradiological Sites
neuroradiology.today
NeuroSience Sites
neuro.science
Neurovascular Sites
vascularneurosurgery.com
Personal Sites
cns.clinic
Spine Surgery Sites
spine.surgery
spondylolisthesis.info
paraplegia.today
Stem Cell Therapy Site
neurostemcell.com

Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses

Multigen RF lesion generator .
|
 |

| | |
|
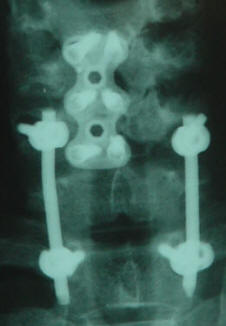
24-MAY-2008 AMAL AL-FAQIR 48 YEARS SLIPPED
UPPER SCREWS IN THE POSTERIOR CERVICAL FUSION DEVICE.
|


Preoperative X-rays showing the construct. |
Anamnesis:
 |
The patient came to the
clinic 05-February-2008 still complaining of
agonizing neck pain and unable to move her left
upper limb. CT-scan performed 05-December-2007
showing good alignment of the four lower screws,
but with partial slipping of the upper two
screws. She was advised to keep in medications
and protelose to accelerate the bony fusion. |
|
|
The patient was advised to be
seen after 4-5 months. |
|
|
MRI lumbar spine performed
22-April-2008 showed good alignment of the
spinal cord and the bony structures, but did not
gave information about the position of the
posterior fusion screws. |
|
|
The patient then came
17-May-2008 and there was some improvement of
her condition, but limitation of the neck
movements and the feeling that the upper screws
are pushing the upper cervical spine anteriorly,
causing massive muscle spasm. |
|
|
The patient was sent for
CT-scan of the cervical spine and simple
cervical X-rays, which confirmed further
slipping of the upper screws. |
|
|
Considering that, a
sufficient time elapsed since the last surgery,
and the necessity of the upper screws is null
and in contrary, they are causing such muscle
spasm and limitation of neck movement, the
patient was advised to undergo partial removal
of the upper third of the construct. |
|
|
In the laminectomy position,
posterior approach was refreshed and the rods
were exposed, just above the level of the middle
screws. The connecting bridge was removed.
Drilling of the rods was performed, as
demonstrated in the postoperative pictures. The
flail screws were removed together with rods. |
|
|
Routine closure of the wound
with smooth postoperative recovery.
|
|
|
The patient showed dramatic
improvement after the surgery, that myself could
not believe in that. With gradual decrease of
pain killers, she kept in good condition and she
was discharged 5 days after surgery. |
Comments
|
|
With the rapidly growing
technologies, new problems arise and with
practice, the good judgment could lead to better
outcome. |
|
|
The posterior fusion device,
as every device has its merits and laps. This
case is a good demonstration, that the slipping
of the upper screws could lead to very agonizing
pain and limitation of neck movement. |
|
|
Such a simple procedure, as
removing the upper third of the device brought
the patient back to normal life. She was
disparate and this condition, including the
previous surgeries caused to her a major
psychological impact. |
|
|
When the patient has
depression and as be seemingly minor morphologic
problem, such as slippage of the upper screws,
do not hesitate to correct the problem. The idea
is to bring all the surgical data to perfect. |
|
|
The patient still showing the
residual of the previous sympathectomy, such as
anhydrosis and warming of the left upper limb.
These manifestation are welcome in her clinical
status. |
Postoperative X-rays showing the acceptable device
positioning.
|
|
|
|
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .
|
|
|
| |