Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
The carpal tunnel syndrome is the
most common entrapment neuropathy. With the report
by Cannon and loves in 1946 of the favorable outcome
in nine patients with median nerve entrapment at the
wrist who underwent carpal tunnel release and
neurolysis, the syndrome became increasingly
recognized. During the next two decades, Phalen
championed and immensely popularized the relatively
simple operation. Carpal tunnel release is now the
most common hand operation performed. Though the
procedure is generally associated with low morbidity
and relatively high success rates, failure of the
surgeon to fully understand the anatomy,
pathophysiology, and typical features of carpal
tunnel syndrome, as well as the many pitfalls
associated with its diagnosis and treatment, may
lead to an unacceptable incidence of suboptimal
results.
Anatomy
The median nerve originates from the
lateral and medial cords of the brachial plexus and
carries in it axons entering or leaving the spinal
cord through the C6,7,8 and T1 nerve roots. It
passes down the arm in the neurovascular compartment
adjacent to the brachial artery but gives off no
branches until the forearm and hand. In the forearm,
the median nerve innervates numerous wrist and
digital flexors of the preaxial muscular
compartment. Though the sensory distribution of the
median nerve in the hand closely approximates the C6
and 7 dermatomes, its motor fibers innervate
intrinsic muscles of the hand within the C8 and T1
myotomes.
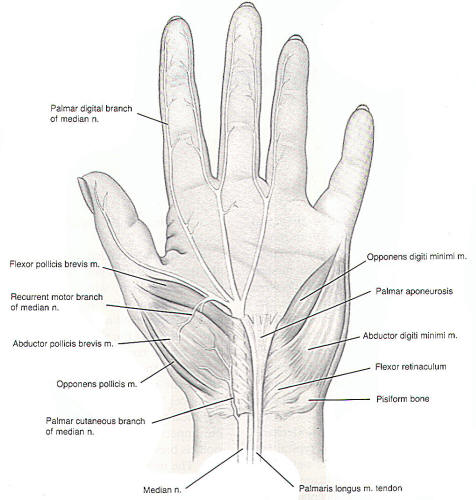
Fig-1: Topographical view of the hand -Anterior view.
1-ulnar n. et a.; 2- flexor digitorum profundus and superficialis; 3- vagina synovialis communis mm. flexorum; 4- median n.; 5- abductor digiti minimi; 6- n. digitalis palmaris proprius; 7- flexor digiti minimi brevis; 8- arcus arteriosus palmaris superficialis; 9- nn. digitales palmaris proprii n. ulnaris; 10- aa. digitales palmares communes; 11- mm. lumbricales; 12- mesotenon; 13- vaginae synoviales tendinum digitorum; 14- vaginae fibrosa digiti manus; 15- aa.digitales palmares propriae; 16- m. interosseus dorsalis I; 17- vagina synovialis tendinis m. flexoris pollicis longi; 18- caput transversum m. adductoris pollicis; 19- nn. digitales palmares proprii; 20- ramus superficialis a. radialis; 21- m. abductor pollicis brevis; 22- m. flexor pollicis brevis; 23- nn.digitales palmares communes n. mediani; 24- ramus muscularis n. mediani.
The abductor pollicis brevis, which
abducts the thumb at a right angle to the palm, and
the opponens pollicis, which flexes and opposes the
thumb, are the most important of the
median-innervated muscles of the hand. These two
muscles of the thenar eminence are innervated by the
recurrent motor branch that typically arises from
the median nerve just distal to the flexor
retinaculum. Damage to this nerve produces loss of
thumb opposition and hence significant difficulties
with grasp. Other muscles innervated include the
superficial (flexor) pollicis brevis and the first
and second lumbricals. The median nerve supplies
sensory fibers to the radial three and one-half
digits via the common palmar digital branches. The
area over the thenar eminence, however, is supplied
by the palmar cutaneous branch, which leaves the
median nerve just proximal to and runs superficial
to the transverse carpal ligament (Figure 1).
Numerous variations in the origin and course of this
surgically important cutaneous branch may be
encountered. The branch may have origin on the ulnar
side of the nerve, or it may course under or through
the transverse carpal ligament.
Fig-1: The median nerve at the wrist.
The transverse carpal ligament, or
flexor retinaculum, is a dense ligament measuring
approximately 4 cm in Width, 5-6 cm in length, and
2.5-3.6 mm in thickness. It stretches transversely
across the concavity of the carpal bones and
converts their arch into a fibrous tunnel. Referred
to as the carpal tunnel, here the median nerve
travels in its most superficial course as
it and a
number synovium-invested tendons pass into the hand.
In 10% of individuals, a small persistent median
artery can be found coursing through this tunnel.
The tendon of the palmaris longus muscle passes
superficial to the transverse carpal ligament and
inserts into the palmar aponeurosis, a tough stratum
of connective tissue that blends into the deep
palmar aspect of the transverse carpal ligament.
This tendon acts as a useful landmark as the median
nerve lies just radial to it. The transverse carpal
ligament acts in part as a paint of origin for the
muscles of the thenar and hypothenar eminences.
Fig-2: Transverse section upper third of the wrist. 1- vagina tendinis m. flexoris pollicis longus; 2- caput superficialis m. flexoris pollicis brevis; 3- retinaculum flexorum; 4- median n.; 5- tendines m. flexorum superficialis; 6- vagina synovialis communis mm. flexorum; 7 - a. et n. ulnaris; 8 - ramus palmaris profundus a. ulnaris et ramus n. ulnaris; 9-m. palmaris; 10- m. flexor digiti minimi; 11. m. abductor digiti minimi; 12- m. interosseus palmaris III; 13- m. opponens digiti minimi; 14- tendo m. extensoris digiti minimi; 15- tendenes m. extensoris digitorum; 16- m. interosseus dorsais IV; 17- tendo m. extensoris digitorum; 18- m. interossius palmaris II; 19- arcus arteriosus palmaris profundus; 20- m. interossius dorsalis III; 21- tendo m.extensoris digitorum; 22- tendo m. extensoris indicis; 23- m. interosseus dorsalis II; 24- The deep fatty space; 25- m. interosseus palmaris I; 26- m. interosseus dorsalis I; 27- tendines m. flexoris digitorum profundus; 28- m. adductor pollicis; 29- tendo m. extensoris policicis longi; 30- tendo m. extensoris pollicis brevis; 31 caput profundum m. flexoris pollicis brevis; 32- m. opponens pollicis; 33 - m. abductor pollicis brevis.
Like the palmar cutaneous branch,
there are numerous variations in the course of the
recurrent motor branch of the median nerve; however,
in
95%
of cases, the motor branch will take one of three
courses. The most common point of origin is the
radial side of the median nerve just distal to the
transverse carpal ligament, frequently arising in
common with the first common palmar digital nerve.
The motor branch then courses directly to the thenar
muscles (Figure 1). The second most common site is
an origination from the median nerve as it travels
beneath the transverse carpal ligament. The branch
then passes around and over the distal edge of the
ligament to the thenar muscles. An origin of the
motor branch from beneath the transverse ligament
with a transligamentous course is the third most
common. In rare cases, the motor nerve may arise
from the ulnar aspect of the median nerve or may
even travel for a short course on top of the distal
edge of the transverse ligament. In cases of
persistent median artery, the median nerve may have
a high division; that is, the motor branch make take
origin many centimeters proximal to the wrist.
Epidemiology and
Etiology
The carpal tunnel syndrome affects
women somewhat more often than men, though the
actual incidence in each sex is not entirely clear.
Fifty percent of cases occur in the fifth and sixth
decades.
Frequently, the patient's occupation will require
repetitive wrist motion or prolonged pressure to the
"heel" of the hand. Recreational-related trauma to
the hand or wrist is increasingly becoming a factor
in development of this entrapment syndrome. Five to
ten percent of all patients will relate a history of
recent or remote injury to the wrist.
Numerous systemic diseases have been
associated with an increased predisposition to
development of carpal tunnel syndrome. Rheumatoid
arthritis, amyloidosis, acromegaly, and
hypothyroidism predispose the median nerve to
compression within the carpal tunnel due to
thickening and hypertrophy of the ligaments and
other connective tissues. The carpal tunnel syndrome
is also more likely to occur in association with
diseases that produce demyelinating or ischemic
neuropathies, such as diabetes mellitus, renal
failure, or alcoholism. Pyridoxine (vitamin B6)
deficiency has likewise been suggested to be an
etiologic factor. Transient symptoms of median nerve
compression are very common during pregnancy and
usually resolve spontaneously after delivery. Any
mass lesion within the carpal tunnel may produce
median nerve impingement, such as neurofibromas,
ganglion cysts, and other benign tumors. Anomalous
muscles and tendons, as well as a persistent median
artery or other vascular anomalies, have been
reported to produce the carpal tunnel syndrome.
Other local conditions, such as synovial
inflammation and fibrosis (as is observed in
tenosynovitis), fracture of the carpal bones, and
thermal injuries to the hand or forearm may be
associated with the carpal tunnel syndrome.
Phalen argues for a common etiology
for many of the idiopathic cases. During the course
of decompressing the carpal tunnel, Phalen biopsied
the synovium of the flexor tendon lying beneath the
median nerve. Chronic inflammation and fibrosis of
the flexor synovialis, consistent with
tenosynovitis, were found in 126 of 148 biopsy
specimens. Phalen also believes a vasomotor
imbalance from sympathetic dysfunction may play a
role in the disease process, though there is no
scientific evidence to substantiate this.
In essence, any disease process that
reduces the cross-sectional area of the carpal
tunnel or increases the volume of its contents may
produce median nerve compression and entrapment,
especially if a concurrent neuropathy predisposes
the nerve to injury from compressive lesions.
Clinical
Diagnosis Symptoms
Carpal tunnel syndrome is
characterized by a typical discomfort and numbness
of the lateral three digits (radial half of the
hand). The pain is often described by the patient as
bothersome "pins and needles" paresthesias, though
occasionally the pain will have more of a deep,
aching quality. The pain may affect the entire hand
or, in atypical cases, radiate proximally into the
forearm, upper arm, or even the shoulder, producing
symptoms that can be confused easily with a C6 nerve
root compression syndrome. The syndrome is
frequently bilateral, though the symptoms are
usually worse in the dominant hand.
A feature quite distinctive of carpal
tunnel syndrome is nocturnal exacerbation of the
symptoms. The patient frequently complains of being
awakened by pain during the early morning hours.
Shaking and massaging the affected hand often
relieve the discomfort. It has been suggested that
akinesia during sleep leads to venous stasis in the
extremities, which exacerbates compression of the
median nerve within the already restrictive carpal
tunnel. By shaking and moving the hands, venous
return is improved, causing a reduction in the
pressure within the tunnel, thus relieving the
uncomfortable paresthesias. Strenuous use of the
hands, especially with repetitive or forceful
flexion movements of the wrist, may also aggravate
the symptoms.
In contrast to ulnar neuropathy at
the elbow, it is unusual for weakness and atrophy to
be present in the early stages of carpal tunnel
syndrome. Thenar atrophy and weakness of thumb
opposition are hallmarks of advanced disease.
Interestingly, the rare patient who initially
presents with weakness and atrophy frequently has
little pain.
Findings
The history alone usually establishes
the diagnosis of carpal tunnel syndrome. Abnormal
findings on neurologic examination may support the
diagnosis in patients with less typical symptoms,
though objective abnormalities are generally sparse
except in more advanced cases. Hypesthesia in the
median nerve distribution may be found, except over
the thenar eminence and base of the palm. This is
due to the palmar cutaneous branch of the median
nerve arising proximal to and passing superficial to
the transverse carpal ligament. This sensory branch
is frequently spared the effects of entrapment
within the carpal tunnel. Motor deficits are seen
less frequently. The two most important muscles
innervated by the distal median nerve are the
opponens pollicis and the abductor pollicis brevis.
The first is tested by having the patient oppose the
thumb to the palm and draw it medially toward the
base of the fifth digit against resistance. The
latter is tested by resisting active abduction of
the thumb away from the plane of the palm.
Significant and long-standing denervation to these
muscles leads to atrophy of the thenar eminence.
Two-thirds of patients will
experience electrical sensations radiating into the
palm and first three digits when the median nerve at
the wrist crease is percussed. This is known as
Tinel's sign, which classically has been associated
with median nerve entrapment at the wrist; however,
recent reports suggest this test to be of dubious
value in establishing the diagnosis of carpal tunnel
syndrome due to a high incidence of false-positive
results in otherwise asymptomatic individuals. A
more accurate predictor of carpal tunnel syndrome is
Phalen wrist-flexion test. The patient is asked to
hold the forearms up in a vertical orientation with
the wrists flexed for 60 seconds. Reproduction of
the patient's painful dysesthesias provides a high
degree of certainty of the diagnosis. Likewise,
inflating a blood pressure cuff placed around the
arm may reproduce the symptoms. Again, symptom
exacerbation in this test is likely due to venous
distention within the rigid confines of the carpal
tunnel.
Electrodiagnostics
Electromyography and nerve conduction
velocities should be obtained to confirm, not to
establish, the diagnosis of carpal tunnel syndrome.
Indications for surgery should not rest solely on
the results of this test, but rather should be based
on clinical judgment. Electrodiagnostic studies are
helpful in differentiating the carpal tunnel
syndrome from other disorders, such as cervical
nerve root impingement or syndromes of the thoracic
outlet.
The most sensitive and the earliest
abnormality found is a prolonged sensory conduction
latency across the wrist. Normally, the distal
latency through the carpal tunnel to the abductor
pollicis brevis is less than 4.5 milliseconds. A
prolonged motor latency generally occurs later in
the entrapment process. The amplitude of the action
potential is frequently diminished. Denervation
potentials in the opponens pollicis and abductor
pollicis brevis indicate advanced and probably
irreversible damage to the median nerve.
Nerve conduction velocities and
latencies are subject to a number of physiologic
variables, such as the age and metabolic status of
the patient, as well as the temperature, vascular
supply, and extent of edema in the arm. Numerous
technical problems are associated with the
determination itself. The treating physician or
surgeon is responsible for being aware of the
variability of the test and for assessing the
results in light of the patient's clinical
evaluation. Should the electrodiagnostic studies be
equivocal, it might be prudent to wait up to 46
weeks to repeat the study before embarking on a
course of surgical management. Though electrical
abnormalities may not be evident in up to 10% of
clinical cases of carpal tunnel syndrome. Many
surgeons will not consider decompression of the
carpal tunnel without electrodiagnostic
confirmation.
Differential
Diagnosis
The surgeon should be aware of the
similarity between carpal tunnel syndrome and other
pathologic processes that cause pain and neurologic
dysfunction of the radial aspect of the forearm and
hand. These include brachial plexopathy from tumor,
trauma, or inflammation, and, less often, thoracic
outlet syndrome. The most common of these, however,
is C6 and C7 radiculopathy caused by cervical disk
herniation or spondylosis. Typically, this pain
seems to originate in the neck and shoulder and
radiates down the arm in a lancinating fashion into
the radial aspect of the hand. Exacerbation of the
pain with movement of the cervical spine is a
significant diagnostic factor in this pain syndrome.
In general, C6 and C7 nerve root compression
produces motor deficits in the upper arm, such as
biceps or triceps weakness, and diminished deep
tendon reflexes. The intrinsic hand muscles are
relatively unaffected.
The median nerve may become entrapped
at locations other than the carpal tunnel. The
pronator syndrome is produced by median nerve
compression at one of a number of locations around
the distal humerus, elbow, and proximal forearm.
Entrapment at these sites produces pain on the volar
surface of the forearm and hypesthesia of the radial
half of the hand. Weakness of the thenar muscles is
observed less often. Symptoms are usually aggravated
by exertion, especially with forceful flexion of the
elbow or pronation of the forearm. Phalen's
wrist-flexion test is typically negative. Likewise,
the anterior interosseous syndrome causes pain in
the proximal forearm. This pain is exacerbated by
exercise and relieved by rest. Because it affects
the anterior interosseous branch distal to where it
leaves the median nerve in the cubital fossa, the
motor and sensory innervation of the hand is not
directly affected, though pain may be referred into
the hand.
Carpal tunnel syndrome may coexist
with other lesions of the nerve roots, brachial
plexus, or median nerve. Concurrent cervical
radiculopathy has been found in over 10 % of
electrically proven carpal tunnel syndrome. This is
referred to as the double-crush syndrome. This
syndrome is based on the concept that proximal
compression of a nerve may weaken the nerve's
ability to withstand a more distal compression.
Management
Nonoperative Therapy
Many cases of carpal tunnel syndrome,
especially mild cases or those that present early in
the evolution of the disease process, are
self-limiting and resolve spontaneously without need
for surgical intervention. In cases related to
systemic illnesses, such as hypothyroidism or
acromegaly, treatment of the underlying illness may
result in improvement or even resolution of
entrapment symptoms.
The occurrence of the carpal tunnel
syndrome in pregnancy is thought to be related to
fluid retention in connective tissues about the
wrist. Nocturnal and exertional dysesthesias in the
radial half of the palm occur in 10% to 25% of
pregnant women. When the carpal tunnel syndrome
occurs, the symptoms are more often bilateral. Onset
of symptoms is typically during the third trimester.
Relief occurs spontaneously, within a few weeks of
delivery, in the majority of cases. Because of its
transient nature, carpal tunnel syndrome during
pregnancy is best treated by using conservative
measures, such as splinting and analgesics.
In the rare case of severe pain
refractory to nonoperative therapy, it is reasonable
to proceed with carpal tunnel decompression using a
local anesthetic. That subsequent pregnancies are
frequently associated with repeated episodes of
carpal tunnel syndrome confirms the association of
carpal tunnel syndrome and pregnancy.
Short-term immobilization of the
wrist by splinting is among the most commonly used
of nonoperative therapies. In general, the splint is
worn only at night, though patients with diurnal
dysesthetic pain should wear the splint at all
times. It is important that the splint be
constructed such that no pressure overlies the
median nerve at the wrist. If symptoms are not
alleviated or improved after 6-8 weeks of splinting.
further conservative management is unproductive. The
patient is then offered the option of surgical
decompression.
Diuretics may prove helpful in
patients with carpal tunnel syndrome related to
excessive fluid retention, such as is observed in
congestive heart failure. Control of hyperglycemia
in diabetics and weight loss in obese patients also
may be of benefit in alleviating symptoms. Adequate
analgesia may be obtained from nonsteroidal
anti-inflammatory drugs. though their long-term
efficacy in the treatment of carpal tunnel syndrome
has not been determined. Pyridoxine administration
has not gained widespread acceptance as a useful
therapy. If development of the syndrome is
occupation related, an alteration of work activities
or even a change of occupation may be necessary.
Much has been written about the use
of corticosteroid injections into the carpal tunnel,
but few objective reports of positive results are
available. Patients with mild and early symptoms
noted a beneficial effect after 3 weeks: however,
those patients with more profound symptoms failed to
respond to this therapy. Others feel steroid
injections may alleviate symptoms though only
temporarily. In the last three decades, enthusiasm
for this treatment modality has waned. Its primary
indication, however, may remain as a means of
controlling symptoms during temporary or reversible
causes of carpal tunnel syndrome, such as is
observed during pregnancy, or following failed
carpal tunnel syndrome surgery.
Administration of corticosteroids
into the carpal tunnel must be precise in order to
avoid injury to the median nerve. A 25-gauge needle
is inserted into the wrist at a point 1 cm proximal
to the flexion crease between the tendons of the
palmaris longus and the flexor carpi radialis and at
an angle of 45 degrees to the long axis of the
forearm. The needle is advanced approximately 1 cm
until the flexor retinaculum is pierced. If painful
dysesthesias in the distribution of the median nerve
are produced, the needle is withdrawn and reinserted
at a slightly different location. One to two
milliliters of a mixture of triamcinolone or a
similar corticosteroid and 1 % lidocaine are
slowly injected. If the patient does not obtain
relief following the first injection, further
injections, in general, should not be pursued.
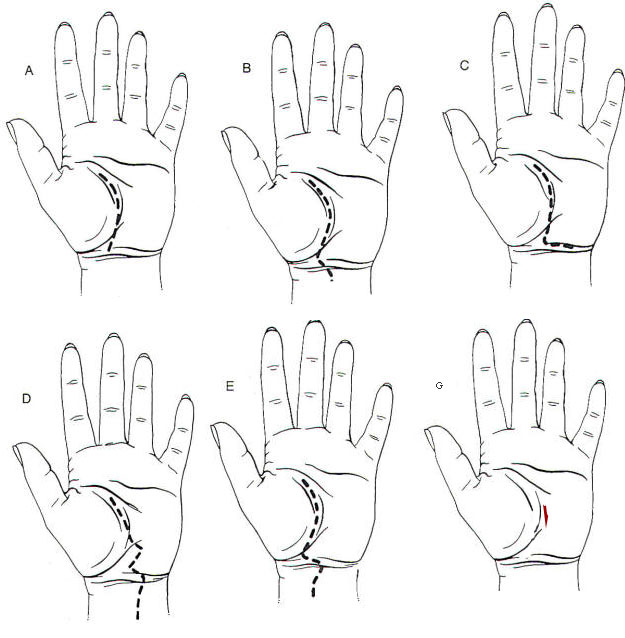
Fig-2: Incisions described by several authors (A-E).
G- The mini-incision in red used by the author.
Surgical Therapy
The indications for carpal tunnel
release are (1) rapidly progressive thenar wasting
and hand dysfunction, or (2) substantial symptoms
that are unrelieved by conservative measures. The
surgeon should be confident of the diagnosis and
have thoroughly excluded other causes of hand
dysfunction and pain.
In cases of bilateral carpal tunnel
syndrome, it is rarely necessary to operate on both
hands simultaneously. The more severely affected
hand (or in the case of symmetric disease, the
nondominant hand) should be decompressed first.
Surgery on the contralateral hand may be performed 6
weeks later, after the first hand has recovered and
has regained full function. Most would agree that
the patient undergoing simultaneous bilateral
procedures would be rendered functionally impaired
and quite dependent, albeit for a short period of
time. Often the symptoms in the less severely
affected hand will spontaneously resolve in the
interim and will not require operative intervention.
One-third of patients with bilateral carpal tunnel
syndrome require bilateral operations. When
bilateral surgery was needed, an interval between
operations of at least 3 weeks was allowed.
Rarely does a patient require general
anesthesia to undergo carpal tunnel release. A
regional block or, if the anesthesiologist is not
well versed in this technique, a locally
administered anesthetic agent is used. The use of a
tourniquet is unnecessary.
There are as many methods of incision
as there are surgeons performing carpal tunnel
releases (Figure 2). The type of incision is of
little importance as long as it follows three basic
guidelines: (1) The incision should be designed to
avoid potential division of the palmar cutaneous
branch of the median nerve; (2) It should be carried
far enough into the palm to confidently divide the
most distal aspect of the ligament in its entirety;
and (3) If it is to cross the flexion crease of the
wrist, it should not do so in a perpendicular
fashion.
A simple transverse wrist incision,
though widely used in the past, is discouraged. This
incision does not offer adequate exposure of the
deep palm in order to ensure that the thickest and
most distal portion of the transverse carpal
ligament has been completely divided. In addition,
the palmar cutaneous branch of the median nerve may
be inadvertently divided, producing numbness over
the thenar eminence or pain related to neuroma
formation. As has been previously and eloquently
stated, "There is no doubt that unless the
transverse carpal ligament is seen throughout its
course, the completeness of division will remain a
matter of hope, faith, and speculation.
Once the incision is made, sharp
dissection is carried through the subcutaneous fatty
tissue to the underlying anterior antebrachial
fascia in the distal forearm and wrist and the
palmar aponeurosis in the hand. Loupe magnification
and headlamp illumination improve the visualization
of anatomic structures. Hemostasis is maintained
throughout the procedure by coagulating and dividing
the small subcutaneous vessels using bipolar
electrocautery. The division of the transverse
carpal ligament begins just radial to this easily
identifiable tendon. Rarely, the palmaris longus
tendon may overlie and appear to compress the median
nerve when the wrist is extended.
The transverse carpal ligament is
sharply divided using a No. 11 blade or fine
Metzenbaum scissors. The division is performed under
direct vision. The incision is made on the ulnar
side of the median nerve where the palmar cutaneous
and the recurrent motor branches are less likely to
be encountered. As the dissection crosses the wrist
into the palm, the transverse carpal ligament
becomes noticeably tougher and thicker. The muscles
of the thenar and hypothenar eminences originate
from the transverse ligament at this site.
Deeper in the palm, the fibers of the
palmar aponeurosis begin to blend with those of the
transverse ligament, thus increasing its thickness
and tenacity. Here it is of utmost importance to
proceed cautiously and with vigilance for an
aberrant course of the recurrent motor branch. A
grooved dissector may be placed beneath the ligament
in order to guide the knife blade through the
tissues. The ligament may be incised likewise with a
scissors throughout its' entire length. The
decompression is incomplete until the transverse
ligament is divided in its entirety. The median
nerve itself is then examined for pseudoneuroma
formation or compression from adjacent masses, such
as neurofibromas or ganglion cysts. The underlying
flexor synovialis is also examined; presence of
severe tenosynovitis is of prognostic importance.
Internal neurolysis or epineurolysis is not
routinely performed unless the procedure is a
re-exploration with the only significant finding
being scarring in and about the nerve. The wound is
then closed with a subcutaneous or subcuticular
absorbable suture, taking care not to reapproximate
the transverse carpal ligament over the median
nerve. Nylon suture is used to reapproximate the
thick palmar skin. Steristrips are placed over the
incision at the wrist and distal forearm. A bulky
dressing is placed and the hand wrapped lightly with
an elastic bandage. It is important that the patient
be reminded to keep the hand elevated above the
level of the heart for at least 24 hours to limit
postoperative edema and venous congestion.
Postoperative
Management
The patient's hand should be bandaged
with bulky dressing material in the palm for I week
after surgery. Active flexion and extension of the
digits as well as thumb abduction and opposition
are encouraged to prevent the effects of prolonged
immobilization. Bulky dressings are discontinued and
the sutures are removed 1-2 weeks after surgery. The
hand is placed back into night splints for the next
few weeks. The patient is allowed to gradually
increase the use of the hand but is discouraged from
strong gripping or other exertional uses until 6
weeks postoperatively, at which time the patient is
allowed to resume full activities. In patients with
significant motor deficits, physiotherapy or hand
rehabilitation is instituted at 4-6 weeks following
surgery.
Generally, relief of painful
dysesthesias occurs almost immediately following
carpal tunnel release. Should the pain and tingling
persist, the possibility of incomplete division of
the transverse carpal ligament or of erroneous
diagnosis should be entertained. A deep, aching
sensation exacerbated by activity may develop in the
thenar and hypothenar eminences and distal forearm
related to swelling at the base of the palm.
Referred to as "pillar pain," the condition is
self-limiting and generally resolves within a few
months. Sensory deficits should show definite
improvement by 6- 12 weeks, though motor deficits
are much slower to resolve. In cases of severe
denervation and atrophy, complete recovery of motor
function should not be expected.
Outcome
Results of
Nonoperative Therapy
One-half
obtain relief of their symptoms with nonoperative
therapy. In those patients unrelieved by splinting
and nonsteroidal analgesics, additional benefit may
be obtained from steroidal injections into the
carpal ligament; however, the effect is generally
only temporary and 65% to 90% of patients undergoing
this treatment modality will experience recurrence
of symptoms.
Results of
Surgery
Relief of pain and improvement in
motor and sensory deficits occur in 90% of patients
undergoing carpal tunnel release. Complete or near
complete resolution of signs and symptoms usually
achieved in 82 % of cases with an additional 10%
obtaining moderate relief. The remaining 8%
achieving little or no relief or worse. Poor
surgical outcomes fall into two main categories: (1)
failure to relieve symptoms and (2) adverse effects
and complications. The former is more common,
probably related to failure to completely divide the
transverse carpal ligament or to adequately manage
other compressive lesions within the carpal tunnel.
A significant number of surgical failures, however,
may be due to misdiagnosis, such as mistaking
cervical radiculopathy, brachial plexopathy, or
diabetic neuropathy for carpal tunnel compression.
This may be especially true if surgical indications
are based on electrodiagnostic tests alone without
appropriate regard for the clinical presentation and
physical findings.
Postoperative failures are classified
into four groups: (1) neurologic complications, such
as injury to the palmar cutaneous branch and other
neural elements, (2) vascular injury, including
palmar hematomas, (3) tendon problems, such as
bowstringing, tendon adhesions, and trigger finger,
and (4) wound complications, including infection,
wound dehiscence, and hypertrophic or painful
scarring across the wrist crease. Except in cases of
incomplete sectioning of the ligament and wound
problems, reexploration following failed carpal
tunnel release may prove disappointing and of
limited benefit.
Avoidance of
Complications
Adverse effects and complications of
carpal tunnel release are under-reported. Only those
authors who deal with a large volume of patients
referred for failure of prior decompressions have
adequate data for evaluation. In a group of
patients, 26 of whom had undergone prior carpal
tunnel release that resulted in postoperative
complications. Fourteen patients had painful
neuromas related to division of the palmar cutaneous
branch, making this the most common complication. In
two patients, failure to relieve symptoms was
related to the use of transverse wrist incisions.
Painful and hypertrophic scarring from perpendicular
wrist incisions was observed in three patients. Two
patients experienced stiffness of the
interphalangeal joints following prolonged
immobilization, two had neuromas of the superficial
branch of the radial nerve, and three experienced
dysesthesia, possibly secondary to reflex
sympathetic dystrophy.In a
series of 186 patients, there were 34 complications
in 22 patients. The complications included 12 cases
of incomplete division of the transverse carpal
ligament (in 8 of these cases, a transverse incision
was used), 11 injuries to the palmar cutaneous
branch of the median nerve, 4 cases of reflex
sympathetic dystrophy, 2 each of hypertrophic
scarring (from perpendicular incisions), palmar
hematoma, and "bowstringing" of the flexor tendons,
and 1 case of adherence of flexor tendons.
Superficial wound infections have been reported to
occur in 0.5 % to 6% of cases. Fortunately, injury
to the recurrent motor branch is a rarely reported
complication.
In analyzing suboptimal results of
carpal tunnel release, over one-half of the patients
evaluated were involved in litigation concerning
Worker's Compensation or automobile, machinery, or
medical malpractice liability.
Retinaculotomy
In 1983, Paine and Polyzoidis
described an innovative method of carpal tunnel
release using a retinaculotome. In their technique,
a small transverse wrist incision is made centered
over the palmaris longus tendon. The flexor
retinaculum is opened medial to the median nerve and
the retinaculotome is inserted. This instrument has
a blunt foot plate beneath a sharp vertically
oriented blade and is designed to acutely incise the
ligament while deflecting the underlying median
nerve. The instrument is passed beneath the
transverse carpal ligament, dividing the ligament as
it is advanced more distally into the palm. The
procedure is repeated in a proximal direction to
divide the remaining ligament. Adequacy of ligament
division is determined by feel and sound, which the
authors describe as being quite characteristic. In
their review of 516 "closed" procedures using the
retinaculotome, 89% of their patients reported
satisfactory results. Their few failures were
thought to be due to incomplete division of the
ligament. Wound hematomas occurred in less than 1%
of the cases. They reported no injuries to the
recurrent motor branch.
Pagnanelli and Barrer reported a
series of 577 hands decompressed using a slight
modification of the Paine and Polyzoidis "closed"
retinacultotomy. Satisfactory results were obtained
in 93 % of cases. Complications were minor and few;
no injuries to the median nerve or its branches
occurred. Length of postoperative recovery appeared
to be shorter with this technique as compared to the
more traditional "open" procedure, and incisional
discomfort was perhaps lessened.
Despite the comparable results
achieved by closed retinaculotomy, it has not gained
widespread acceptance among surgeons performing
carpal tunnel release. However, the limited
experience with this innovative technique challenges
surgical dogma that the transverse carpal ligament
must be divided its entire length under direct
visualization. Further experience is needed to
evaluate the role of this procedure in the surgical
treatment of carpal tunnel syndrome.
Summary
Carpal tunnel syndrome is a common
affliction, especially among persons whose
occupations require repetitive wrist motion.
Numerous systemic disease processes can predispose
to the development of this disorder. Symptoms are
quite characteristic as are physical findings;
however, because of occasional similarity between
other nerve compression syndromes, electrodiagnostic
tests may be necessary to confirm the diagnosis of
carpal tunnel syndrome. Early and mild cases are
frequently self-limiting and resolve with time or
conservative measures. This is especially true with
regard to pregnancy-induced carpal tunnel syndrome.
Symptoms are adequately managed in one-half of the
cases by using wrist splinting, analgesics,
physiotherapy, and occasionally steroid injections
into the carpal tunnel. In those cases unrelieved by
nonoperative means, surgical decompression of the
carpal tunnel can be undertaken with an 80% to 90%
success rate. Surgical failures can be minimized if
care is taken to avoid injury to the palmar
cutaneous and recurrent motor branches of the median
nerve, and if an incision is made that avoids
hypertrophic scarring in the wrist yet allows
adequate visualization for division of the distal
extent of the transverse carpal ligament.
With a proper understanding of the
anatomy, pathophysiology, clinical presentation, and
available treatment modalities for median nerve
entrapment at the wrist, the surgeon can expect to
offer substantial relief to the majority of his or
her patients afflicted with carpal tunnel syndrome.
For more than twenty years, the carpal tunnel release got a standard technical standard with an incision maximum 10-12 mm length, ulnar side of the main crease only 2 mm. away from it. The incision could be smaller, but the available smallest self-retaining retractors govern the length of the incision. There is no need to have special marks during the performance of the incision. It is preferable to palpate the area to get the feeling where the retinaculum flexorum is located. It has variable location. Some have low-positioned localisation, others have a high one. The important point is to put the incision 3-4 mm. above the lower border of the retinaculum. Using blade No 11 the incision is done down to the retinaculum, where no muscle is seen. The lower edge of the retinaculum is identified and incised with blade, after what the fat and the nerve are under visual control. To achieve that the lower end of the incision is retracted down by minirectactors. The most compressed part of the retinaculum must be incised by blade without insertion of a scissors, to decrease the surgical trauma. All is done with direct vision and within the fibrotic part, where all the time no important structures are seen. Even with the use of above elbow tourniquet, arteriols must be coagulated to avoid postopertative bleeding. After releasing the most compressed part of the retinaculum, the wound retracted the wrist and with blunt small-tipped scissors the final part of the retinaculum is released. Using Mack-Donald blunt raspatory the canal is checked up to 4 cm above the wrist for evidence of stricting bands. The nerve is inspected, but not violated if it has no pathologic lesions. Two absorbable subcutaneous stitches and subcuticular closure routinely performed. Compressive crippe-bandage used for 24 hours to avoid hematoma formation. It happened that, the nerve was tumorous and resection of the tumor was performed. But this must be planned before surgery. For the simple CTS, it is a bad idea to violate the nerve. I have seen even operated upon neurosurgeons by orthopaedists with unnecessarily violated synovial sheets with series of complications. Even if the synovial structures were hypertrophied, release of the nerve is sufficient. Over 1000 operations were performed during the 25 years with prompt disappearance of the numbness and no complications were encountered.