Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
08-MAY-2012 FATMEH AHMAD AL-TMESHAN 48 YEARS
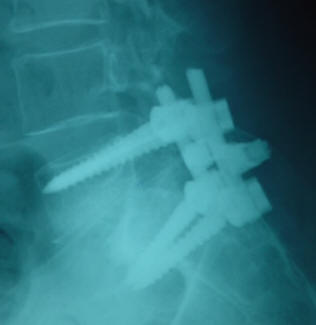
III DEGREE SPONDYLOLISTHESIS L5-S1.
Anamnesis
The
patient came to the clinic 10-April-2012
complaining of LBP for 5 years with right
sciatica for one year and bilateral sciatica for
5 months with numbness both feet, more big toe
territory with intermittent claudication and
inability to walk more than 100 meters. The
patient is a known case of diabetes mellitus for
15 years.
MRI lumbar
spine performed 10-April-2012 showing
assimilation of D10 and 11 with III degree
spondylolisthesis L5-S1 .
On
examination, the patient is limping, dragging
the right lower limb with exaggerated scoliotic
stance. SLRS was 30 degrees in the right with
pain and 60 degrees in the left with pain.
Planterflexion both feet was 4/5 and
dorsiflexion right foot -3/5 and left foot 3/5.
There is hypalgesia both L5 and S1 territories.
Skeletonization of L4, 5
laminae down to the lateral processes. Laminectomy
of L5 with removal of all flail parts of the
lateral masses and the isthmolytic parts of the
pedicles. Foraminotomy of L5 and S1 roots both
sides. The L5-S1 disc space is unreachable due
to severe degree of spondylolisthesis. Insertion
of monoaxial Spineway transpedicular screws to
the L5 bodies 7x40 mm. During insertion check
X-ray and inspection of the L5 roots was
considered. Insertion of Reduction
polyaxial screws 6x35 mm were inserted to S1
body with inspection of the S1 roots and under
image-intensifier. The insertion was bicortical
because the screws available were the shortest.
The rods were inserted and reduction distraction
was applied, after what it was possible to
perform discectomy L5-S1 and insert TLIF cage 8
mm height with NeveBone. Slight
compression was applied to prevent slippage of
the cage. Bone chips were inserted in the disc
cavity. CrossLink 55-70 mm was applied. The bone
chips were applied to the rods.
Routine
closure of the wound. Smooth postoperative
recovery.
Please! wait for 3-5 min till the
video start to load. It depends upon the internet
connection.
Comments
The patient has III degree
of spondylolisthesis with bilateral isthmolysis.
Surgical correction and fixation is the only
solution at our present time.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .