Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
21-AUGUST-2014 FATMEH SALEH AL-DROOBI 20 YEARS
RECURRENCE OF HIGHLY MALIGNANT GLIOMA RIGHT CONVEXITY.
Anamnesis
The patient was operated by me
04-July-2013 for highly malignant glioma,
followed by radiotherapy and chemotherapy. The
patient then came 18-August-2014 complaining of
headache the last 2 weeks with tinnitus right
ear and numbness left upper and lower limbs
coming as Jacksonian sensory marsh.
MRI brain done 07-July-2014 showing mass over
the tentorium right side with cystic component
reaching the right ICA bifurcation.
On examination; the patient is neurologically
free.
The patient was sent for new MRI of the brain
with contrast with MRA of the brain and
spectoscopy, DTI and functional MRI and done the
same day. The results of investigations shown in
Fig. 1-6, listed below.
The incision was refreshed and extended more to
the base and the old bone defect removed and
further bone flap created to gain adequate
access to the tentorial plain. The solid tumor
attached to the tentorium in the right side was
removed in piece-meal fashion. It was highly
vascular with pathologic vascularity. Inomed
ISIS was used to study the sensory motor area
through the dura. The area is far from the
operative activity site. The posterior parts of
the temporal lobe were involved in the
resection. The medial edge of the tentorium was
seen and resection was limited so as not to
violate the interpedincular cistern. After
getting the impression that the tumor was
totally resected, the patient was sent for MRI
control. There are still 2 masses over the
created cavity. Spectroscopy done to them. See
fig-7. The
choline level was low in the cavities, but the
mass under then is an active tumor. Despite this fact, these
2 masses were removed. The medial part was
abutting the right internal capsule. These
cavities were containing yellowish fluid. Strict
hemostasis and routine closure of the wound.
Smooth postoperative recovery. The patient
extubated immediately and she is moving the left
side of the body and responding well. There is
left side hemiparesis, more the leg.
Comments
The patient is young, underwent
radiotherapy and chemotherapy. In the last
preoperative MRI with spectroscopy there is still places
were active tumor recurrence aside with radionecrosis. It
was decided to remove the active tumor parts with the
radionecrosis to give the patient the maximum chance of
survival.
The more radical the resection, the more
favorable outcome, but this governed with possible
complications, even of you use the most sophisticated
technology.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
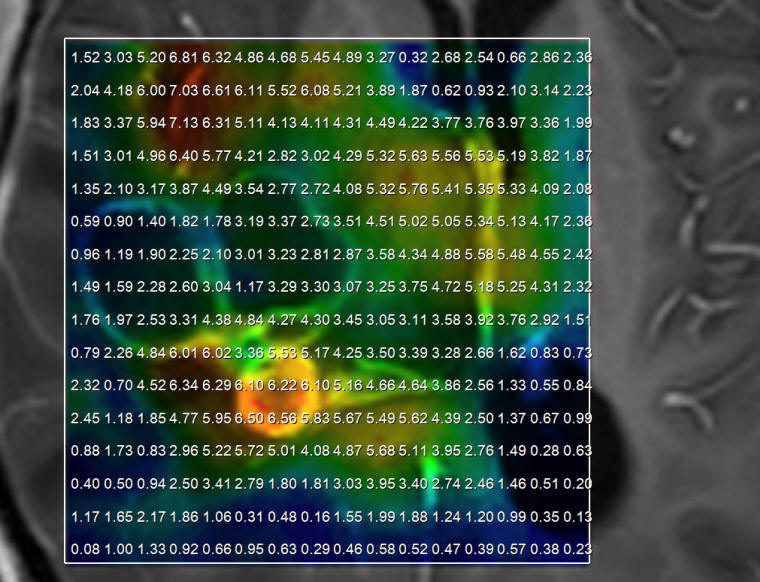
Figure-1: Choline still high in some places confirming the
recurrence of the tumor.
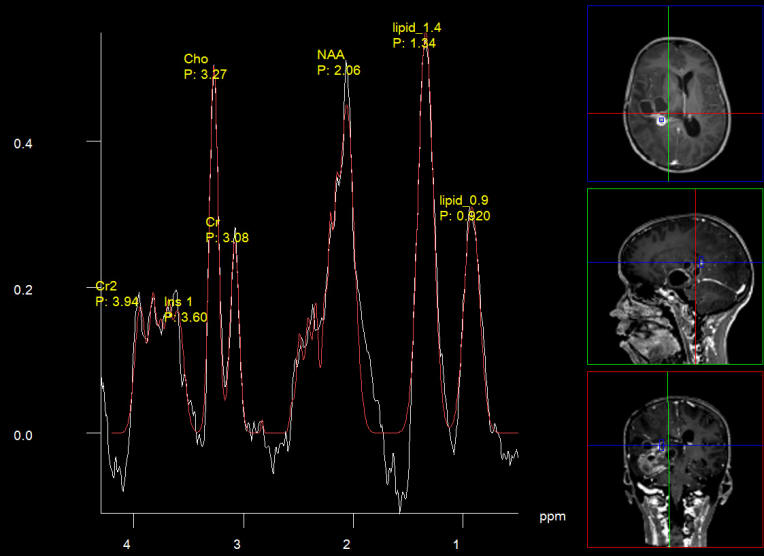
Figure-2: Short TE showing also the presence of lipids 13 and
9.
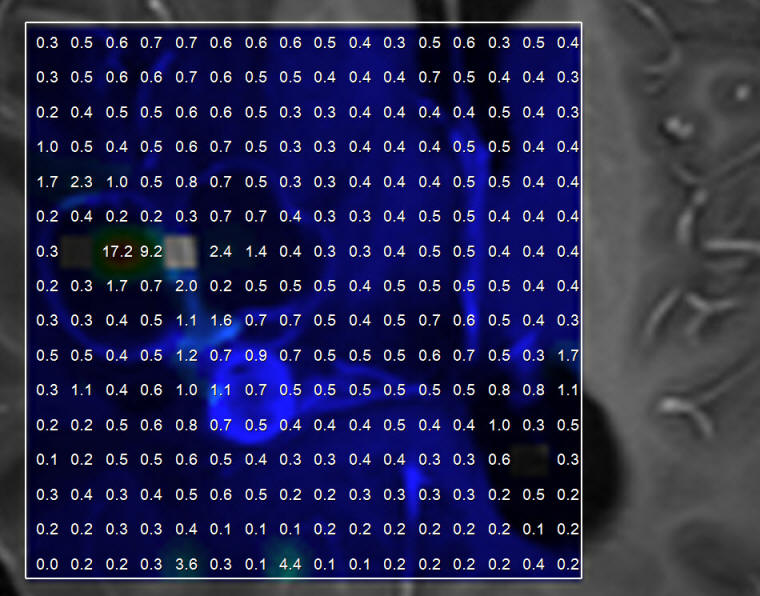
Figure-3: Choline to NAA ratio distribution.
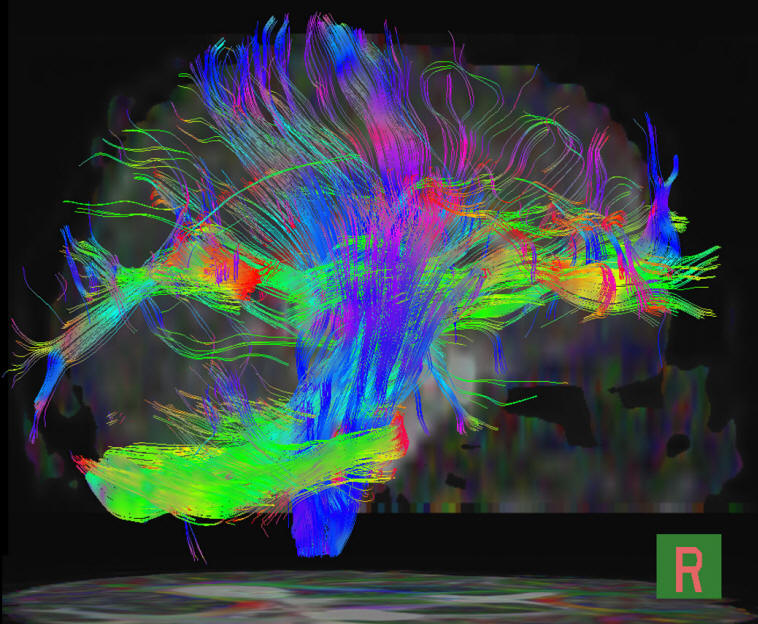
Figure-4: Fiber tracking showing missing fibers above the tentorium
in the right side.
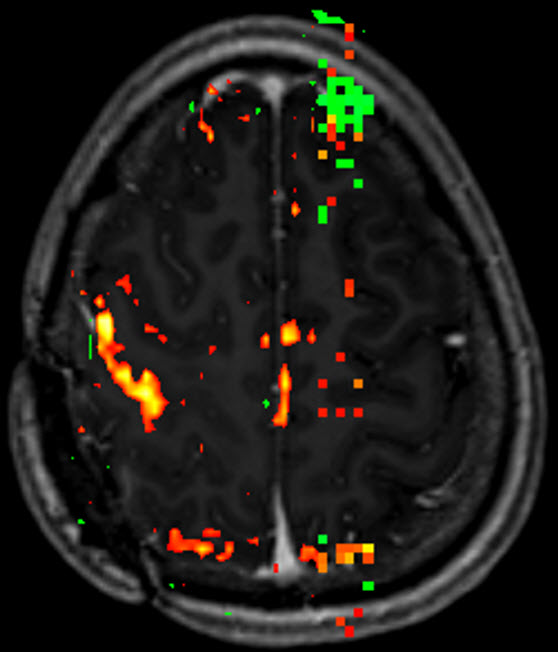
Figure-5: Functional MRI showing functioning left side of the body.
Figure-6: Sagittal plane showing the mass shifting the brain stem
and other structures.
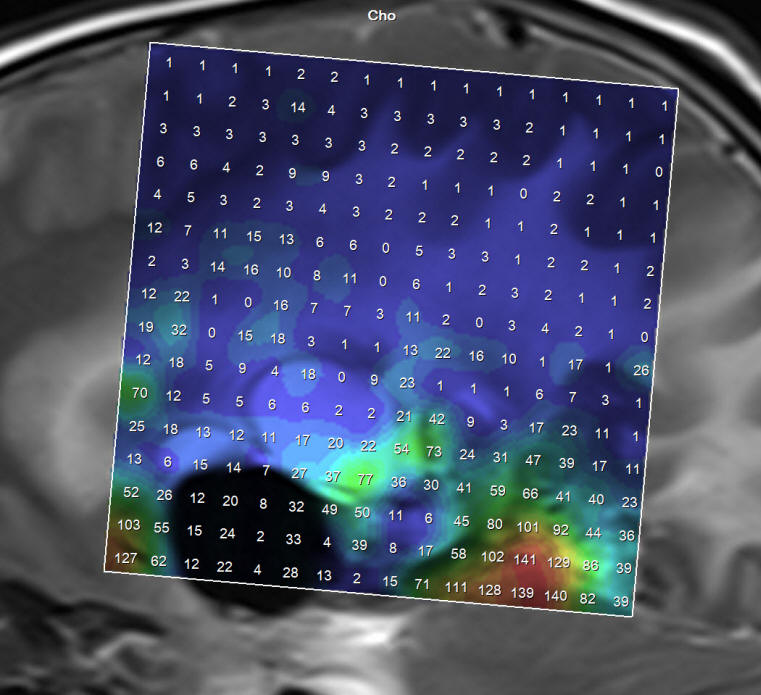
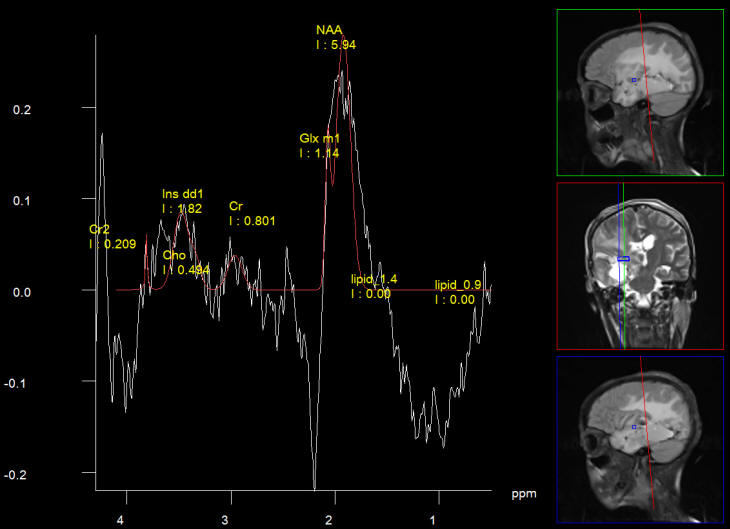
Figure-7: Intraoperative spectroscopy showing remnant of active
lesion below the cystic lesions, which are abutting the internal
capsule.
During surgery we use saline and the air come to fill the cavities
and an error message coming out during spectroscopy telling that
fluid suppression is an adequate. Despite this fact it is possible
to catch the active remnants and establish the fluid content of the
cysts.
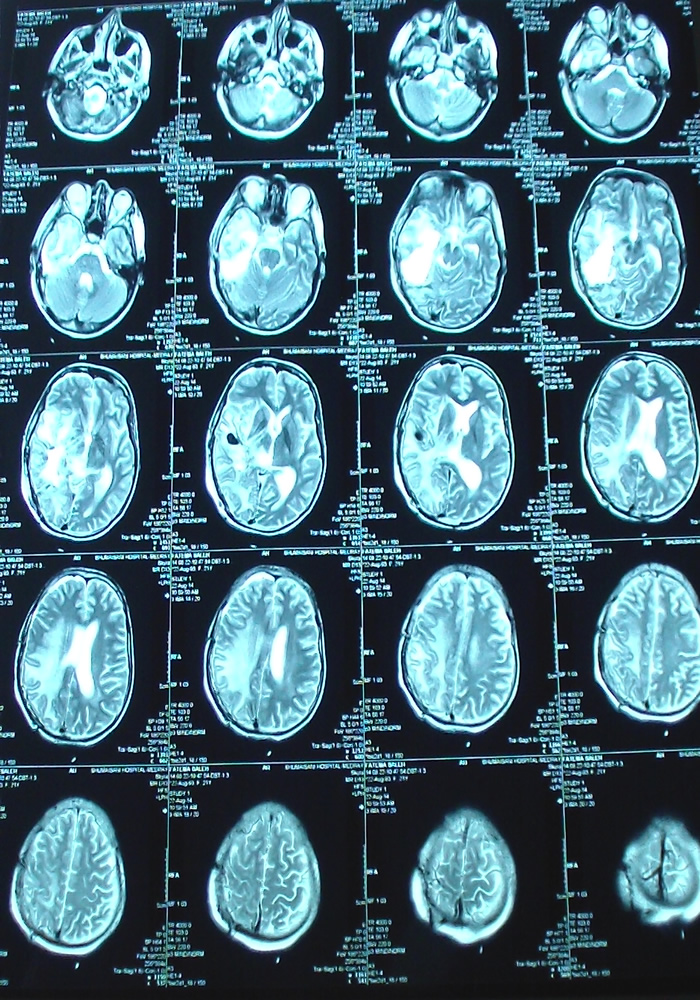
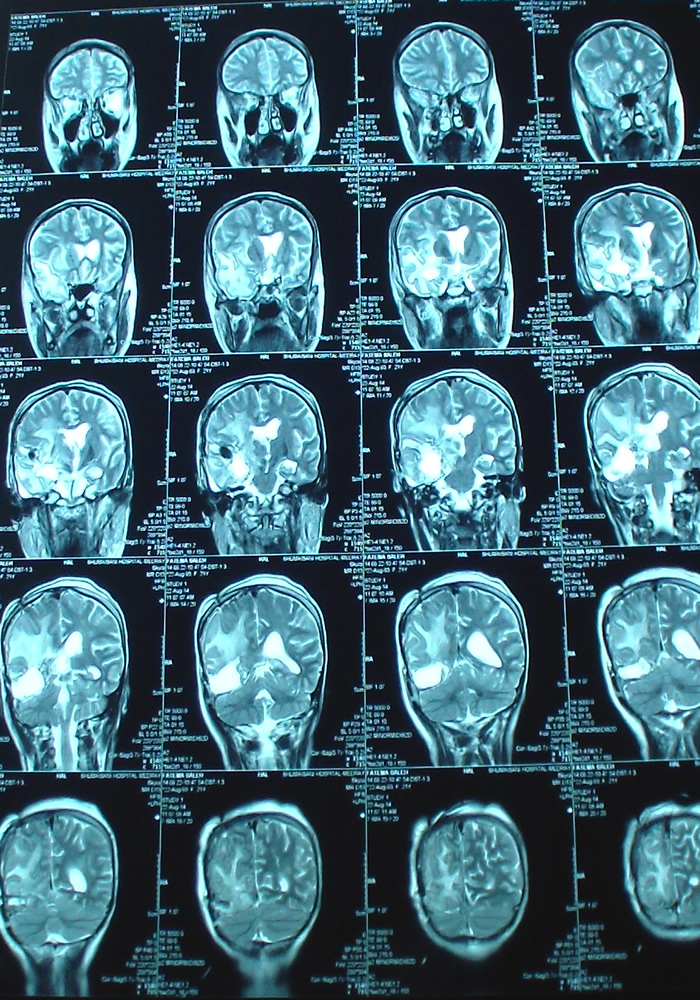
Axial TW2 done the second postoperative day.
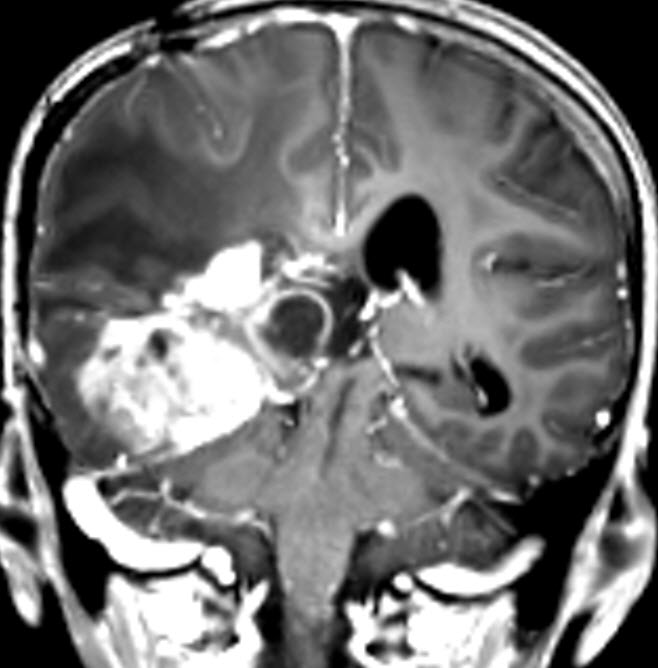
Coronal MRI done the next postoperative day. Notice how near the
dissection to the right internal capsule.
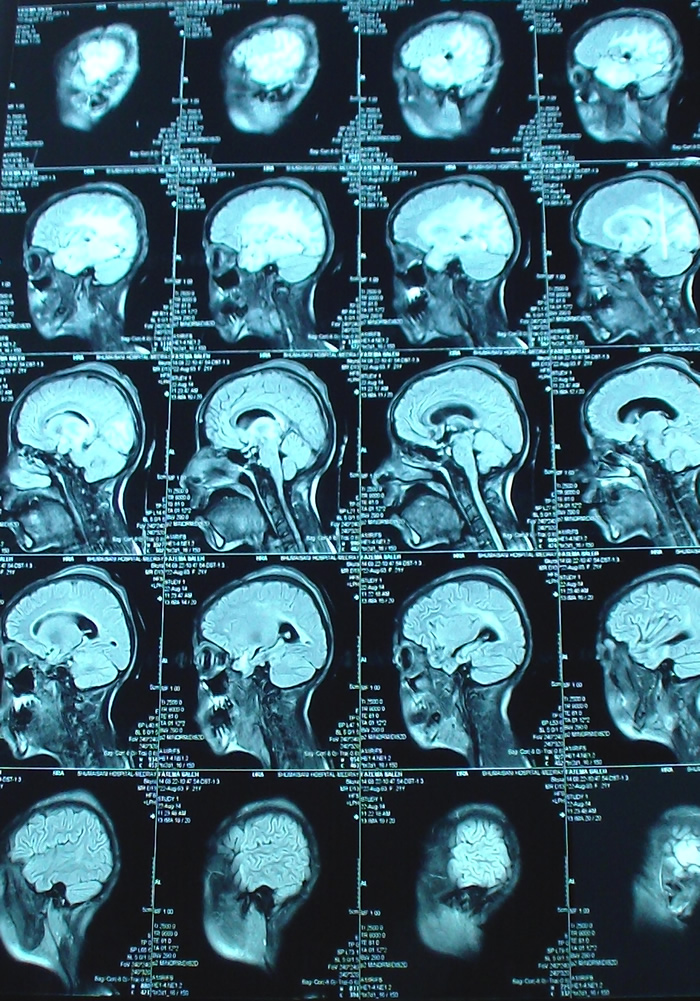
Sagittal TW1 done the next postoperative day. Notice the
radical resection, in comparison to the MRI done during surgery.
Spectroscopy done the next postoperative day, showing the
absence of tumor and the chemical shift of the internal capsule,
which was seen during surgery and it was respected. This is the
first time in my life seeing the internal capsule during
surgical dissection.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .WELCOME
TO AL-SHMAISANI HOSPITAL