Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
17-AUGUST-2014 FIRAS AZZAM AL-TMEZEH 29 YEARS
BILATERAL ACOUSTIC SCHWANNOMAS WITH PROGRESSING RIGHT SIDE.
Anamnesis
The patient came to the clinic 09-January-2010
complaining of V1 pain for one month and
decreased hearing right ear for 2 years. MRI of
the brain performed 05-January-2010 showed right
acoustic schwannoma extending to the brain stem
and left intracanalicular one. Audiometry done
07-January-2010 confirming practical hearing
loss in the right side. Tegretol was started and
the patient came 14-April-2010 telling that he
was neuralgia free with medication and the pain
resumed when he stopped it. The patient was
advised to keep in medication and to be followed
later. The patient came 19-July-2010 with MRI of
the brain done 18-July-2010 showing the same
tumors sizes and the neuralgia is not present.
The patient came several times over the years
and he was reluctant for surgery. The last time
he came 07-August-2014 and sent for new MRI
which was done the same day. There is
enlargement of the right acoustic schwannoma,
compressing the brainstem. The right mass
25x19x17 mm and the left 20x10x9 mm.
On examination; the patient neurologically the
same as before.
In setting position, midline incision with curve
to the right. Osteoplastic craniotomy over the
right cerebellar hemisphere, with bone defect
abutting the transverse and right sigmoid sinus.
The tumor was identified and using Inomed system
the facial nerve was identified running anterior
and superior to the tumor mass. The
glossopharyngeal nerve was pushed downward.
Piece meal resection of the tumor was carried
out until the intracanalicular part was seen.
The tumor mass was rubbery, highly vascular and
adherent to all tissues in the surround, even
with the facial nerve. The facial nerve was severely adherent to the
intracanalicular part, for what a small residual
was left to keep the function of the right
facial nerve. Check of the function of the right
facial nerve at the stage, which seemed to have
practical radical removal of the tumor, showed
good response of the nerve. The patient was sent
to MRI, which showed a part of the tumor still
hanging under the tentorium. The patient was put
back to the setting position and the remnant of
the tumor was removed in one piece. Strict
hemostasis with application of surgicele. The
wound was water-tightly closed and the patient
was sent another time to the MRI. The mass is no
longer seen, instead a small hematoma with
acceptable brain stem was seen.
The patient was extubated immediately after
surgery. Smooth postoperative recovery with deep
paresis of the right facial nerve.
Comments
The patient had the opportunity to have
Inomed intraoperative control and MRI control during
surgery. Despite the fact that the right facial nerve was
responding well after completing manipulation around it, the
patient showed deep paresis of the right facial nerve.
Removal of the intracanalicular part will certainly
completely destroy the anatomical structure of the facial
nerve.
MRI help in identifying the missed part
of the tumor, which was removed after the first performed
MRI .
The second MRI after completion of
surgery and before extubation was to see the condition of
the brain stem, so as to plan what to do the next step: put
the patient in ventilator or extubate him. Since the
brainstem was in good shape the patient was immediately
extubated Fig1-2.
This case demonstrate that MRI must be
performed at regular basis after surgery to prevent
escalating complications, which could evolve several hours
after surgery Fig 3-4.
Even with the advanced technique,
complications will remain, but the facial nerve recovery
will be judged over the time.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
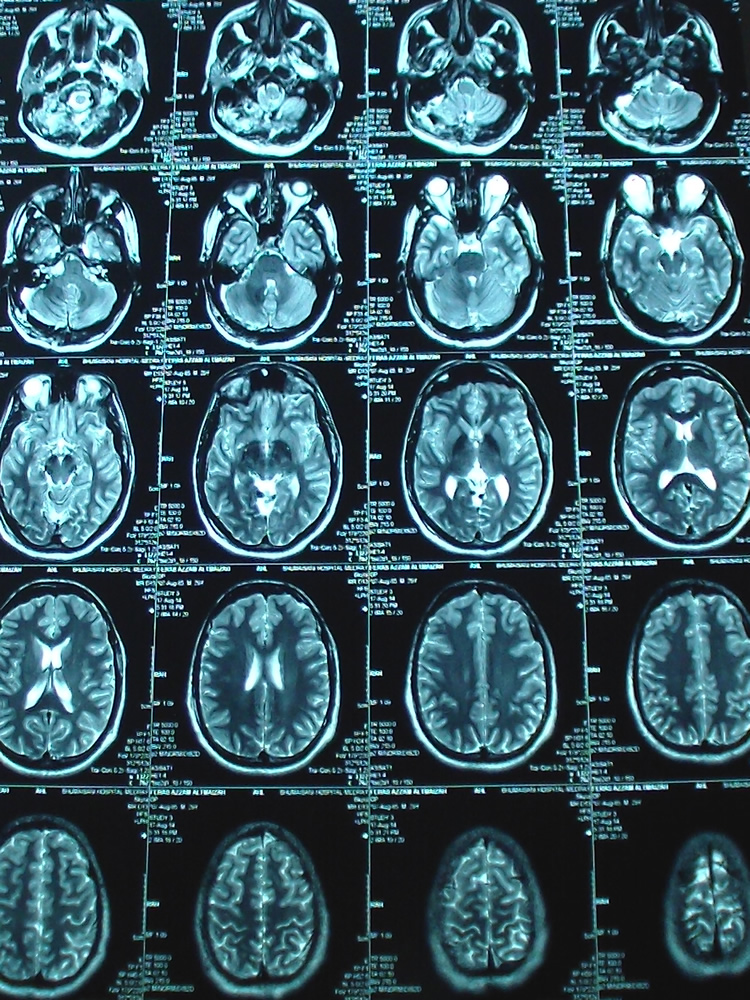
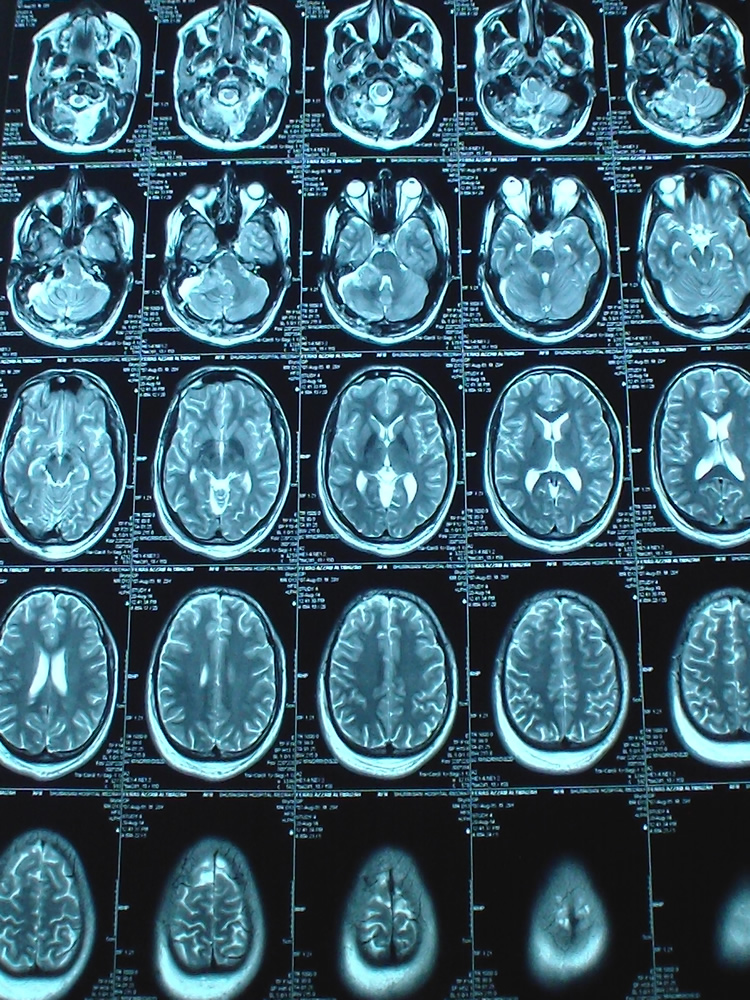
Figure-1: Axial TW2 done during surgery showing the removal of the
residual mass which was stuck to the pontomedullary junction.
Figure-2: The intraoperative TW1 MRI showing the clearance of the
right acoustic schwannoma without any edema or infarction at the
resected last part f the tumor.
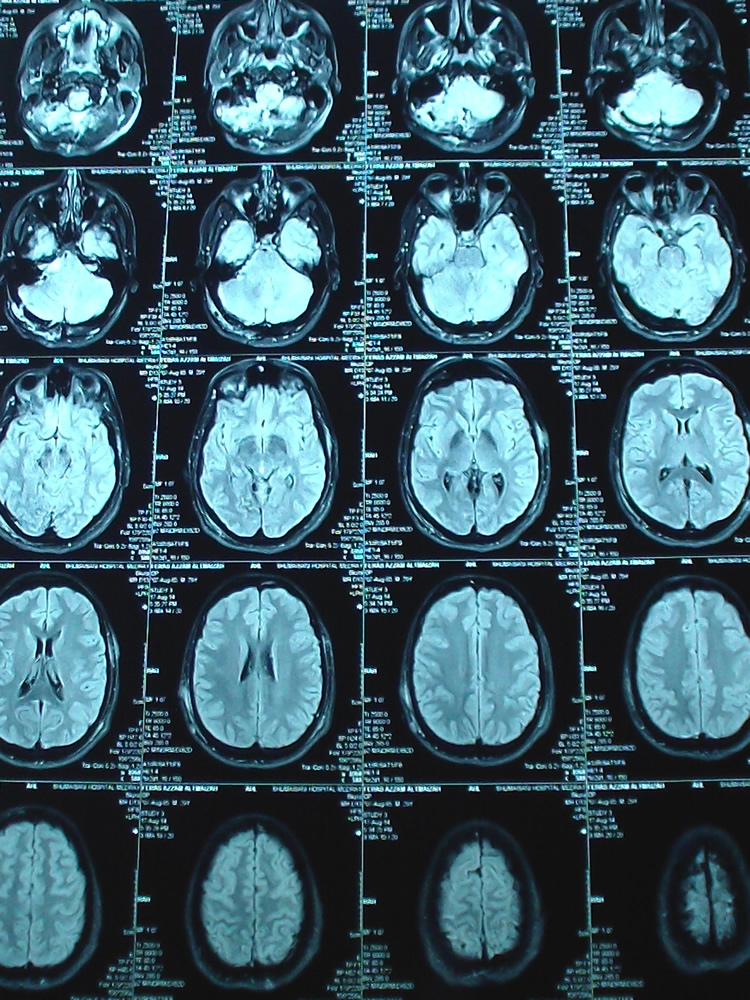
Figure-3: TW2 MRI done 2 days after surgery, demonstrating the
progression of edema at the resected last piece of the tumor. which
was severely adherent to the medullo-pontine angle.
Figure-4: Coronal TW2 done 2 days after surgery showing the edema,
which evolved several hours after surgery.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .