Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
25-DECEMBER-2019 GHALIEH QREYTAN AL-WADHI 44 YEARS
HUGE PROGRESSING MASS INTRADURAL AT C1-2 WITH FULL BLOWN BROWN-SEQUARD SYNDROME
LEFT SIDE.
Anamnesis
The patient came to the clinic 21-November-2019
complaining inability to walk the last 3 years
with weak four limbs, more the left and
hypalgesia from the right C4 down. MRI of the
cervical spine bad quality,
not complete study performed 27-December-2017
showing intradural mass behind C1-2 23x14.7 mm
in dimension with severe edema of the spinal
cord down to C5.
On examination: there is weak both deltoids
-4/5, right biceps 4/5, grip right hand
4/5, left hand 3/5, extensors both hands 3/5.
both biceps 3/5.
Weak dorsi and planterflexion right foot 3/5,
left foot 2/5, both quadriceps
femoris 4/5 and left iliopsoas muscles 2/5.
There is analgesia below the right C4 dermatome.
Deep reflexes S>D with Hoffmann more brisk in
the right. Babinski positive right side and
bilateral clonus more brisk in the left foot.
Defecation and micturition preserved.
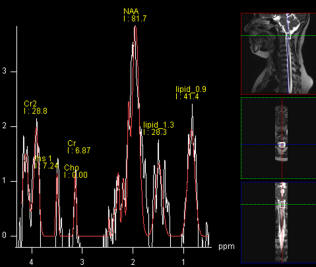
The patient was sent for investigations
with complete protocol of MRI with clinical
applications, including fibertraking and
spectroscopy, which were done
21-November-2019 showing huge meningioma
occupying the intradural space 28x14.7 mm with
matrix of the tumor anterior. Spectroscopy ruled
out malignant nature denoting meningioma
character of the lesion.
In Concord position with
the head maximally flexed down, trying to
avoid CSF coming from the intracranial cavity,
laminectomy of C1 and C2 was performed and the
posterior rim of the foramen magnum was drilled out. The dura was
opened and the edges reflected to the sides.
Inspection around the spinal cord ruled out presence
of meningioma or exophytic tumor. The tumor was seen
through a very thin layer of the spinal cord of the
right side of the spinal cord. Sharp dissection of
the spinal cord over the tumor longitudinal to
expose the tumor. Piece meal resection of the tumor
and part was sent for histologic studies and using
SONOCA 300, some parts of the tumor were resected.
There is calcification inside the tumor, which were
used as landmark for tumor resection. The NVM5 was
used with MEP which showed after start of the
surgery failure to record activity from the left
side, which was actually not violated. Using
MultiGen bipolar stimulation both sides were
responding at the grid areas. The procedure was
undertaken without using muscle relaxants and the
patient could move the right side of the body.
Strict hemostasis after ensuring total removal of
the tumor. The patient was checked by MRI and no
residual of the tumor was seen. Routine closure of
the wound.
Smooth postoperative recovery.
There is dense plegia of the left extremities. She was sent to the
ICU.
MultiGen
Follow Up
The patient in the ICU at 19.00 after receiving
50 mg Pethidine, got loss of consciousness and
blood gas was performed showing high level of
CO2. The vital signs are acceptable and it was
planned to keep monitoring. The morning of next
day, chest X-ray showed cardiomegaly and patchy
chest. Repeat MRI showed improvement of the
surgical site with normal brain. Cardiologist
confirmed presence of myxoma and the patient was
put in ventilator to resolve the CO2 narcosis.
After correction, the patient regained
consciousness and was planned to keep her in
ventilator for three days.
A trail to put the patient with extubation was
tried 29-December-2019, but the patient asked to
put her back to ventilator after one hour.
Tracheostomy size 8 was performed the morning of
30-December-2019.
At the morning of 03-January-2020 the patient
progressed difficult breathing and at 13.00
the tracheostomy was inspected and it was half
away out. Trail to reinsert it and replace it
failed and surgical emphysema with severe
bronchial spasm took place. Cardiac arrest and
brain death was recorded at 13.30.
Comments
This case is challenging with its severe
compression of the spinal cord at C1-2 level with practical
quadriparesis and left sided para-aneasthesia below right C4
dermatome.
It is mandatory to keep the patient under
IOM at all stages of surgery, trying not to touch the
severely compressed spinal cord.
In this case the tumor turned to be an
intramedullary tumor, for what the spinal cord was violated
at its thinnest part to expose and remove of the tumor.
Logically speaking the tumor must be in
the left side, but it turned to be located at the right.
In retrospective analysis the tumor
bigger mass was compressing the right side of the upper part
of the crossing of the pyramidal tract.
The histologic result was consistent with
schwannoma.
This is the 192d case using MultiGen in
the lateral aspects of the spinal cord, which confirmed
presence of connectivity to both girdle muscles at
stimulation around 1.2 V both sides.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Inomed Riechert-Mundinger System, with three point
fixation is the most accurate system in the market. The microdrive and
its sensor gives feed back about the localization.
Inomed MER system
Leica HM500
The World's first and the only Head mounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
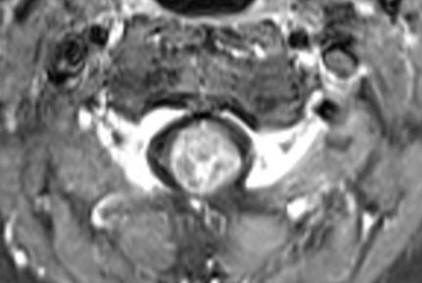
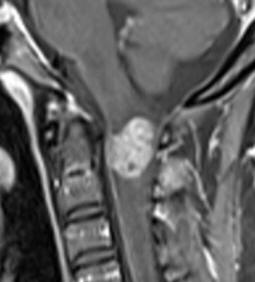
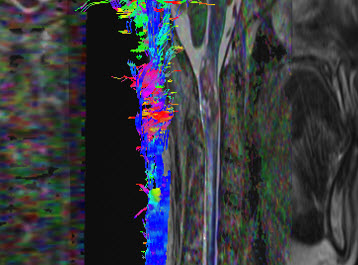
Fig.1: The mass and it relation with the spinal cord. Notice the
fibers are still preserved in the left side of the mass.
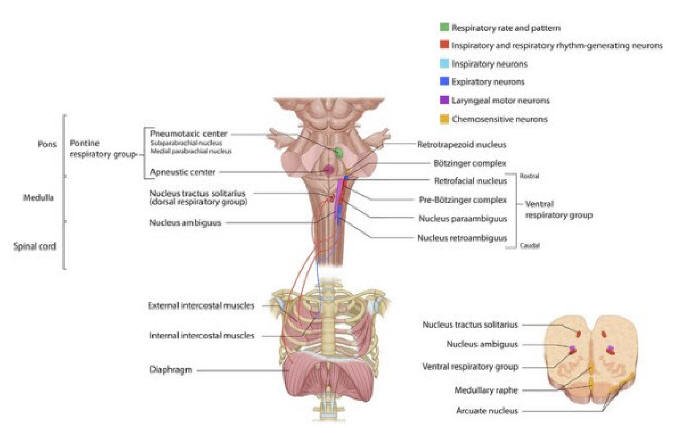
Fig. 2. Central control of respiration. The pontine respiratory
group, consisting of the pneumotaxic center and the apneustic
center, provides tonic input to the medulla to control smooth
respiratory rhythm. The apneustic center, which inhibited by the
pneumotaxic center, delivers excitatory input to the pre-Bötzinger
complex. Receiving sensory information from peripheral
chemoreceptors and pulmonary mechanoreceptors, the dorsal
respiratory group of the nucleus tractus solitarius controls
inspiratory muscles through output via the phrenic nerves (emerging
from the phrenic motor nuclei at the ventral horn of cervical spinal
cord levels C3-C5) and external intercostal nerves. Much like the
dorsal respiratory group, the rostral portion of the ventral
respiratory group provides output to the inspiratory muscles.
Conversely, the caudal portion of the ventral respiratory group
provides output to the expiratory muscles via the internal
intercostal nerves. With permission of Sardar Ali Khan.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .