Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
20-DECEMBER-2017 HAMZEH SALAH AL-JAABARI 36 YEARS
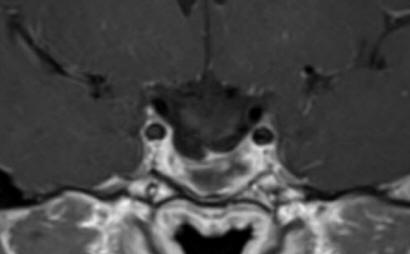
HUGE PITUITARY ADENOMA WITH MASSIVE INFRASELLAR AND MODERATE SUPRASELLAR
EXTENSION.
Anamnesis
The patient came to the clinic 14-December-2017
complaining of blurred vision left eye for three
years. The last week go almost blind left eye
with decreased vision right eye. MRI done in
Turkey 11-December-2017 showing huge pituitary
adenoma with massive infrasellar and moderate
suprasellar extension with signs of apoplexy of
the tumor bed with fluid level inside the tumor.
The patient is convulsion free.
On examination, the patient can feel the light
in the left eye and can count the fingers around
1 meter before the right eye. The oculo-motor
innervation is intact. There is no galactorrhea.
Normosmia. There are manifestations of
panhypoptuitarism, but no data for diabetes
insipidus.
The patient was sent for thorough
radio-ophthalmo-endocrine investigations. MRI of
the sella with MRA done 16-December-2017 showed
the tumor pushing the chiasm and optic nerves
with suprasellar extension around 16.2 mm. The
tumor has massive infrasellar extension reaching
the naso-pharyngeal space abutting it. The tumor
dimensions are 37.3x28.6 mm. There is no
invasion of the cavernous sinuses. There is
fluid level inside the tumor confirming the
presence of apoplexy. Visual acuity of the right eye after
correction 6/6. The left eye 6/0.05. There is
massive scatoma left eye with less in the right
eye. Prolactine 470 ng/ml, LH 1.19, testosterone
0.3. Considering the above data trans-sphenoidal
approach with MRI control was advised.
Mathematically speaking the volume of the tumor
with the hypophysis is around 8.8 ml.
The patient was put in
setting position to perform trans-sphenoidal
approach with the C-arm projecting to the sella
turcica. A trial to evacuate the tumor by
epidural needle 14 was attempted and brownish
content was achieved. The patient was sent for
MRI control. The tumor still there with new
bleeding inside the evacuated cavity. The
puncture site was extended and the rubbery
pituitary inferior wall was incised. The
tumor was removed using curettes for biopsy and
the remaining was removed by suction. It was
possible to see the posterior borders of the
pituitary gland. Using Omnipaque diluted
3cc was injected to the tumor cavity. It is
pulsating well, manifesting the absence of
suprasellar part of the tumor. The patient was
sent another time for MRI control. The tumor
practically resected with the pituitary stalk
hanging free and the optic nerves more than 8 mm
above the superior surface of the preserved
pituitary gland. There is no bleeding inside the
cavity. Routine closure with tampons of
nostrils.
Smooth postoperative recovery. The
patient was sent to the ward.
Comments
The patient can be operated
intracranially, but the massive infrasellar extension is
hard to detect through such angles, even with endoscopic
facilities.
This postoperative course of
transphenoidal approach is smooth in comparison to
subfrontal approach.
The tumor configuration dictate the
proper approach.
For more details about trans-sphenoidal
approach click
here, please.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Inomed Riechert-Mundinger System, with three point
fixation is the most accurate system in the market. The microdrive and
its sensor gives feed back about the localization.
Inomed MER system
Leica HM500
The World's first and the only Head mounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
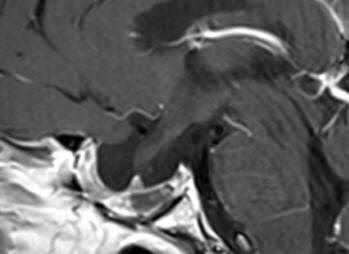
Fig:1- Follow up MRI performed 14-January-2019 3 months after
completion of radiotherapy.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .