Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
19-NOVEMBER-2015 HUDA ABDALLA HAYDARA 45 YEARS
GIANT WIDE BASED PLANUM SPHENOIDAL AND TUBERCULUM SELLA MENINGIOMA WITH HUGE
SUPRA-RETROSELLAR GROWTH MORE TO THE LEFT.
Anamnesis
The patient OS A Yemini lady came to the clinic
14-November-2015 complaining of blind left eye
for 3 years with bifrontal headache for 2 years
and almost blind right eye for 8 months.
On examination; the patient is blind in the left
eye and can differentiate fingers 10 cm near the
right eye. The right eye shift lateral when
looking anterior with horizontal nystagmus when
looking to the right.
The patient was sent for investigations and MRI
done 14-November-2015 showing a giant meningioma
involving the planum sphenoidale and tuberculum
sella with massive supra-retrosellar growth more
to the left with left optic nerve canal
extension and stretching with spasm of the left A1 and edema
of the left frontal lobe.
Bifrontal craniotomy with
reflection of the bone flap to the right. The
frontal sinuses were violated and the mucosa
stripped accordingly. The dura was opened
parallel to the base of the anterior fossa and
both olfactory tracts were dissected of the
mediobasl frontal lobes, but the left one was
completely destroyed by the tumor and it was not
possible to dissect it to the trigone for what
it was intentionally bisected to remove the
anterior part of the tumor. The tumor was rich
in feeders and it was necessary to remove it by
piece-meal fashion after coagulation. That part
compressing the right optic nerve was removed,
but at the junction with the chiasm, the tumor
was stuck with optic nerve, for what a tiny
layer was lift intentionally to preserve the
right optic nerve. That part which was extending
to the left optic canal was removed, but a thin
layer stuck with left ICA was left to avoid
vasospasm. It was coagulated. The tumor was
followed posteriorly until the basilar artery
was seen with Liliquest membrane has defect due
to tumor invasion. Most of the time dissection
was carried at the area of the right A1 segment
and the tumor was maximally removed. It was
possible to expose the chiasm at its medial
part, which was pushed posterior. The area of
the left A1 segment was not violated and to
avoid possible bleeding from this segment, a
surgicelle was applied to this area. All the
feeders which were many, were coagulated and
bisected by microscissors. Strict hemostasis and
routine closure of the wound with repair of the
frontal sinuses by muscle harvested from the
left thigh. The patient was sent MRI to
investigate the circulation, since a lot of
vascular dissection was carried out, especially
the right side. MRI showed severe spasm of the
left ICA at the bifurcation from the left CCA.
MRI with contrast showed branched of the left M1
and the left A1. This could be due to transitory
spasm. The patient then was extubated.
Smooth postoperative recovery. The patient
showed at the start right side paresis, which
resolved over minutes. She was
sent to the ICU for 24 hour observation.
Follow Up
The patient progressed right sided paresis with
pronounced spasticity 2 hours after surgery. The
next day the right limbs improved and the
spasticity gone, but she developed diabetes
insipidus for what Minirin was started. She
still have total aphasia.
Studying the tumor using ORS Visual
Comments
The tumor is very huge with blind left
eye for three years. There recovery of the left eye mostly unpredictable,
but the improvement of the right is mostly predictable.
Intraoperative MRI not only confirm the
radical removal of the tumor, but also detect other events
such in this case.
Arterial spasm after release of the
stretched arteries must be anticipated and treated
accordingly. Nimotop was started the day before surgery.
Intraoperative MRI confirmed the
escalation of such event, but surprisingly the spasm got
place in the left ICA distal to the junction with CCA. I was
afraid of right circulation compromise, but got the opposite
site. This can be explained to gross vascular dissection and
the exposure of the basilar artery with slippage of clots
around it or the surgicelle which was put to the left side
to avoid manipulation with the left A1.
This is the most difficult meningioma I
have ever seen. Thousands of feeders and invasion of the
arteries and the neural tissues surrounding the area. The
operation took 10 hours which is not long to me. Some other
operations took 30-40 hours, but here the character of the
tumor restricting to go further.
For more detailed information about
arterial spasm, please click
here!
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Inomed Riechert-Mundinger System, with three point
fixation is the most accurate system in the market. The microdrive and
its sensor gives feed back about the localization.
Inomed MER system
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
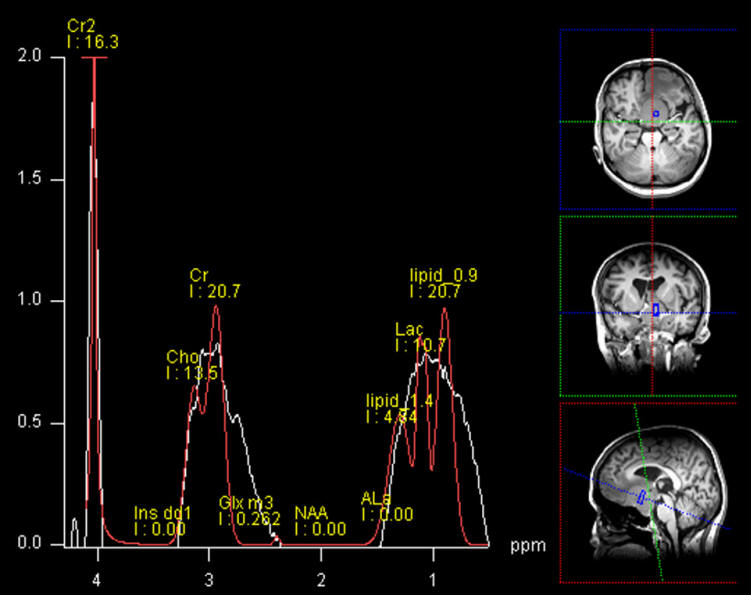
MR Spectroscopy showing absence of NAA and high CR and Cr2. No signs
of malignancy could be detected.
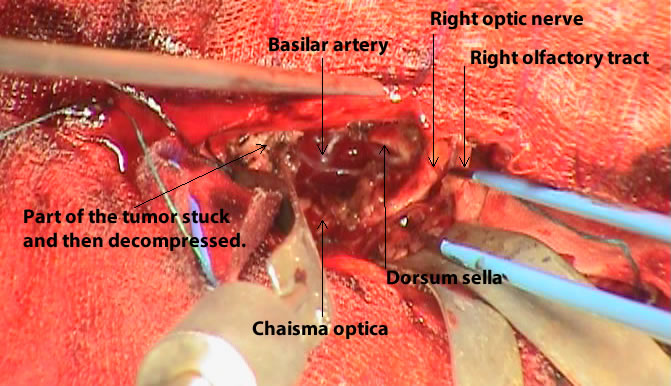
One frame from the video showing the anatomical structures before
the end of surgery.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .