Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
25-JUNE-2013 HUSSEIN ALI AL-QADI 53 YEARS
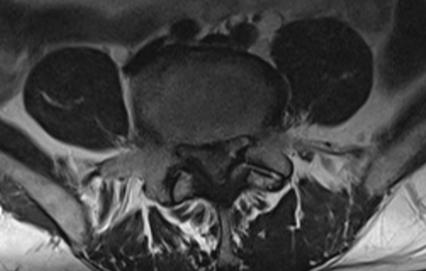
HUGE EXTRUDED DISC L4-5 WITH RIGHT DOWNWARD MIGRATION AND CAUDA EQUINA SYNDROME.
Anamnesis
The patient came
to the clinic 24-June-2013 complaining of LBP
for 4 years. The last 2 weeks
got exacerbation of LBP with bilateral sciatica
more the right with numbness all toes both feet
more the right
and dripping of urine and constipation, for what
Foley's catheter was inserted 2 weeks.
MRI lumbar spine done 16-June-2013 showing huge
extruded disc L4-5 with downward migration
bilateral more to the right. Dorsal MRI was
normal.
On examination: The patient is limping with
mild scoliotic stance. SLRS was 80
degrees with minimal pain in the right. Weak
dorsiflexion right foot 3/5 and left foot 4/5.
Weak planterflexion right foot 1/5. There is
hypalgesia both L5 roots and left S1 and
analgesia right S1 root territories.
Bilateral L4-5 flavotomy and
foraminotomy both L5 roots. The ligamentum
flavum was swollen and severely compressing the
neural structures. The extruded disc even it is
pushing the axilla of S1 laterally, but it was
impossible to attack it from under the axilla,
because of absence of true anatomical borders to
reach it. It was decided to reach the L4-5 disc
space and perform discectomy so as to reach the
extruded disc, which was reached and pushed to
the intradiscal space and removed in one piece.
After that the axilla and dural sac became lax
and free. Inspection of the left L5 axilla
revealed acceptable alignment. Meticulous right
sided intradiscal cleaning of L4-5 disc space.
Routine closure of the wound.
Smooth postoperative recovery.
The power of left foot dorsiflexion became normal
and slight improvement of the planterflexion and
dorsiflexion
right foot.
The extruded disc in MRI causing cauda equina.
Comments
The patient still has an estimated postoperative
recurrence around 7%, because the disc space is
still not shallow, even with bilateral cleaning.
Recovery of urination and defecation needs
several weeks after decompression.
When the extrusion is huge and SLRS is
acceptable, then separation of the sequester
from the annulus fibrosis is the case. In case
of still continuous with the annulus fibrosis
more compression of the axilla upon motion will
trigger more pain.
The patient has bed sore at the sacral area,
which hold suspicion about the real story of his
illness. It must be in more protracted period of
time.
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .