Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
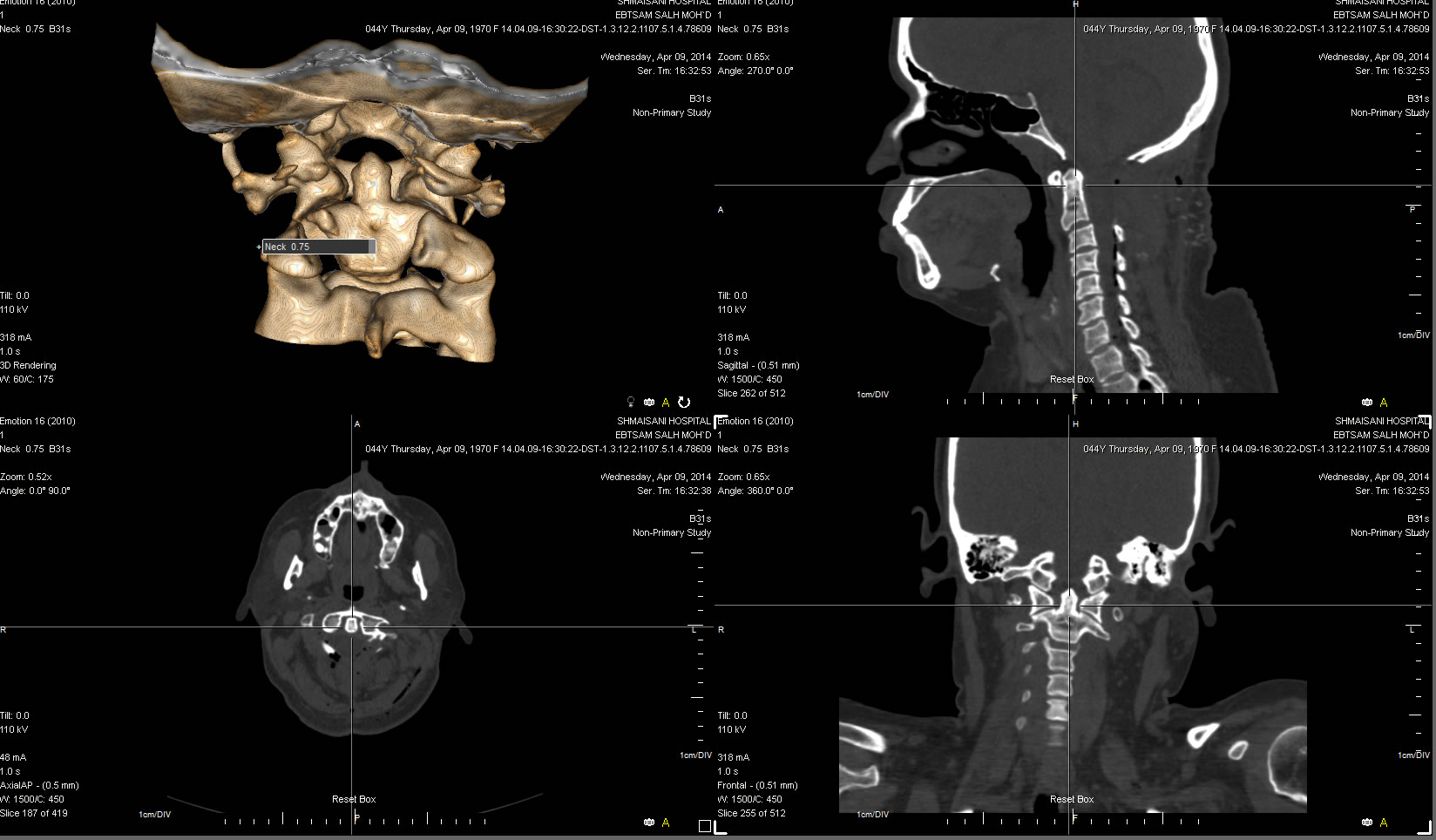
09-APRIL-2014 IBTISAM SALEH HAMAD 43
YEARS BONY TUMOR OF THE C1 LAMINA LEFT SIDE WITH SEVERE SPINAL CORD
COMPRESSION.
Anamnesis
The patient came to the clinic 10-March-2014
complaining of LBP for 18 months with right
sciatica for 4 months down to all toes right
foot. She has occipital headache for 1 month. MRI
cervical spine done 04-March-2014 showing an
osseous bony tumor originating from the left
side of the C1 lamina with severe compression of
the spinal cord. MRI lumbar spine showed bulge
L5-S1 disc.
On examination; the patient is not limping. SLRS was
60 degrees both sides without pain. Romberg
stable with no cerebellar signs. There is weak
left upper limb and both feet and the proximal
muscles of the left lower limb 4/5. Babinski was
positive both sides. MRI of the brain with MRA
ruled out presence of any connection with the
vascular structures.
Setting position. Skeletonization of the foramen
magnum, C1 and C2 laminae. Drilling around the
lesion, which was involving the left half of C1
and C2 laminae and forming a joint between the
C1 and the foramen magnum. There was a joint
between the pathologically changed C1 and C2
laminae in the medial and left parts of the
laminae. The drilling was continued until the
dura was seen all around. Elevation of the
compressing bony mass, which was adherent to the
dura. Sharp dissection was done to avoid
traction tear of the dura. The dura of the
spinal cord after completion of the elevation of
the bony mass became lax and hanging free. There
was a joint between the left half of C1 and C2
laminae and between the lamina of C1 and left
side of the foramen magnum. The mass was sent
for histologic studies. The left C1 root was
seen. The left vertebral artery was seen within
its canal at the C2 level. The left C2 root was
seen in the lower left corner of the created
bony defect. Checking for instability with the
setting position with DORO fixed clamps is
impossible. Using the C-am in the lateral
position with 25 degrees rotation to both sides
also gave insufficient data to rule out
instability. Using the C-arm in AP in the
setting position also was impossible.
Further dissection of the left lateral bony
parts with manual inspection gave bony
continuity of C1-2 for more than 20 mm,
confirming the presence of sufficient stability.
Routine closure of the wound.
Smooth postoperative
recovery. The power of four limbs became normal.
It was decided to perform
CT-scan of the area to
have more confirmation about the stability of
the bony structures.
Immediate postoperative CT-scan confirming the stability
of the construct.
Comments
The patient has a bony mass of unusual
morphology. The mass in consistency is bony hard
but is different from healthy bone. It is more
vascularized and having abnormal joints between
the C1 and C2 laminae and the C1 and foramen
magnum.
The lesion is causing clinical
deterioration. May be the deformity is
congenital and with age start to manifest
itself. The histologic result will clear the
situation.
The final histologic result confirm the presence
of normal bone and bone marrow. This means, that
the patient has this rare congenital anomaly.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .