Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
11-DECEMBER-2014 IBTISAM SAEED ISMAEEL 65
YEARS INTRAMEDULLARY EPENDYMOMA AT D9-10 LEVEL.
Anamnesis
The patient came to the clinic 02-December-2014
complaining of back pain for 8 months with
numbness both feet last 2 weeks.
On examination, the patient is not limping with
mild scoliotic stance. The left AJ is absent.
There is weak dorsiflexion left foot 4/5. There
is pain during percussion of the lower dorsal
spine.
The patient was sent for MRI of the dorsal and
lumbar spine. MRI lumbar done the same day
showing huge cyst right kidney and bulge L3-4
and L4-5 disci. The dorsal spine showed
intramedullary mass extending from D9 down to
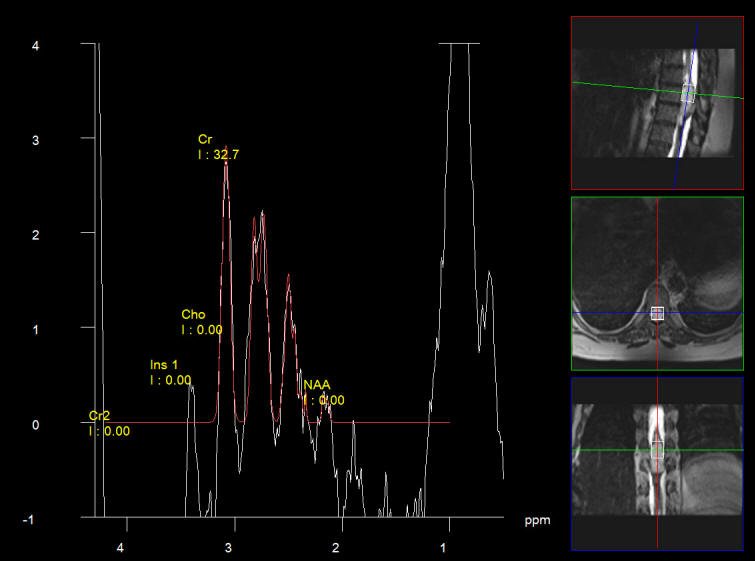
D10. Spectroscopy and DTI were performed and
shown below.
Laminectomy D9,10 and partial of D8 and D11. The
dura was opened. The tumor was seen under the
surface of the medulla and it was expanding it
to all directions. A small parallel to the
midline incision were the tumor was seen was
done through which a golden fluid came out.
Attempt to remove the tumor through this small
incision failed because the tumor was stuck to
all walls of the spinal cord cavity. It was
necessary to extend the posterior incision all
over the tumor to achieve practical total
removal. Inomed lumbar spine protocol was used,
but it was troubleshooting, for what
transpedicular set was used instead. The
roots above and at and below the resected tumor
were functioning. The wound after meticulous
hemostasis was closed and MRI of the tumor bed
was done confirming total resection of the
tumor.
Smooth postoperative recovery.
The patient moving both lower limbs with more
weakness in the right leg.
Follow Up
The patient after surgery cannot walk, despite
the fact that the power of both lower limbs
became normal. On examination there is
hypalgesia of the right anterior thigh for pain
light touch and temperature. The left foot is
colder than the right. The deep reflexes are
present both side more brisk in the right. She
has bilateral disturbed. The 2 point
discrimination is not achievable over all the
body, which made it hopeless in the clinical
evaluation. The conscious muscle joint sense is
disturbed both sides more in the proximal
muscles of the legs. We could make her walk 3-4
steps the 3d postoperative day and aggressive
physiotherapy is undertaken.
Comments
The patient was bleeding all the time and
after mutual conflict with the anaesthesia staff, they were
told to decrease the patient high blood pressure and to give
her Vit K 10 mg. after what it became more possible, but
still difficult to work.
Fibertraking is misleading in
pathological anatomy in the brain and spinal cord. This case
failed to show the real thickness and distribution of the
spinal cord fibers.
The entire tumor capsule was adherent to
the spinal cord. It was necessary to perform long posterior
incision, which can cause more neurologic sequelae.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
Inomed MER system
Spectroscopy showing low NAA with low choline which is in favor for
low grade ependymoma.
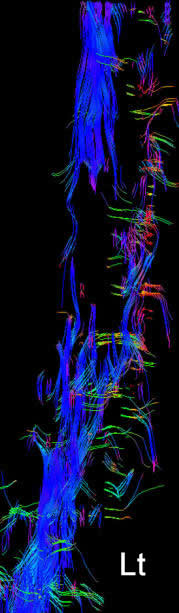
Fibertraking of the spinal cord around the lesion in anterior first,
left second, posterior third and the last is right projections
showing the fibers more concentrated in the left side, despite the
fact the patient has weak left foot.
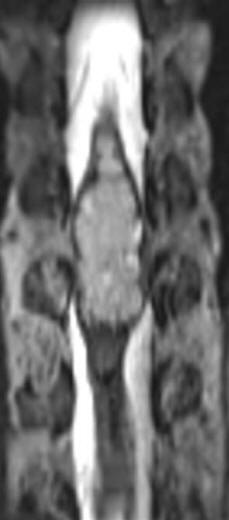
MRI in coronal and sagittal sections showing the tumor before
surgery
Intraoperative MRI Sagittal showing radical removal of the tumor.
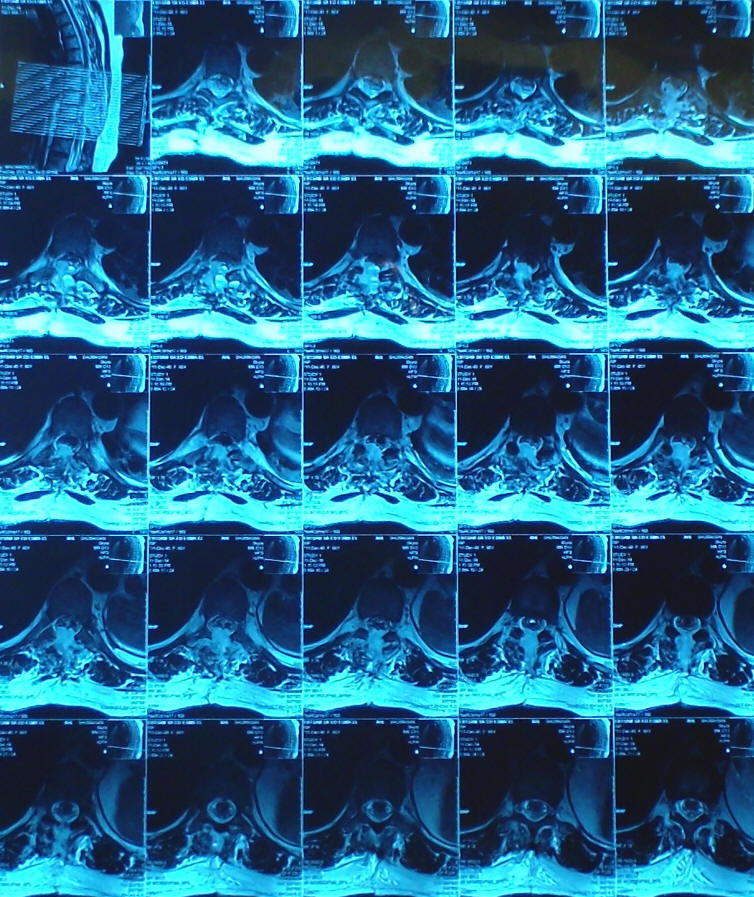
Intraoperative MRI axial views showing that the spinal cord mass was
mainly in the left side supporting the fibertraking data.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .