Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
19-OCTOBER-2017 INAAM UQLAH KASSAB 72 YEARS
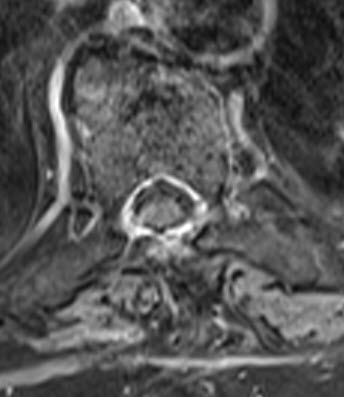
HUGE MENINGIOMA WITH SEVERE RIGHT EXTRAMEDULLARY COMPRESSION AT D7 LEVEL.
Anamnesis
The patient came to the hospital 18-October-2017
bedridden. She suffered fracture of the right
ankle 1 year ago, for what P.O.P was applied.
The last 7 months she started to suffer of
difficulty of walking with loss of urination and
defecation control. The patient performed
elsewhere MRI and reported as having glioma of
the spinal cord at D7 level. She is a known
diabetic for 15 years under treatment.
On examination, the patient is in bed with
inability to walk, nor set down. Examination of
the cranial nerves and neck was unremarkable.
There is para-aneasthesia below the nipples.
There is severe spastic both lower limbs with
difficulty to move the limbs more spastic the
right one. Dorsiflexion right foot was 0/5 and
left foot -3/5, the same with planterflexion.
Abduction left knee was -3/5, but abduction of
the left knee and movements of the right knee
was 0/5. Quadriceps were difficult to evaluate.
SLRS was 0 degree in the right and 3 degrees in
the left. KJ was exaggerated in both sides and
absent in the left side, Babinski positive both
side with clonus right foot and very spastic
both lower limbs. There is ulceration in the
right side of the lower back.
The patient was sent for investigations and MRI
dorsal spine showed meningioma 3.3 x1.3 cm in
diameter pushing the spinal cord to the left,
extending from the D6 down to D7. CT-scan of the
dorsal area was performed for the surgical
planning.
Laminectomy of lower half of D6, D7
and upper half of D8 under guidance of the C-arm.
The upper border was full of epidural fat, for
what it was believed that we were at right
level. The dura was opened and inspection of the
spinal cord from all corners was normal. The
patient was sent for MRI and the tumor was
locating 3-4 mm above the upper border of the
exposed dura. Laminectomy of the above vertebra,
where the epidural fat was hypertrophied with
arterialized veins. The dural incision was
extended up, until the upper border of the
meningioma was seen. About 1/3 of the tumor came
out off the dura from the right side and the
matrix of the tumor was coagulated. Step-wise
resection of the tumor with resection of the
right D7 bridging root to avoid traction injury
to the spinal cord. The tumor was totally
resected without touching the spinal cord, which
by time started to have normal appearance. Using MultiGen, bipolar motor stimulation of the
right side of the spinal cord below the resected
tumor
was achieved with 0.7 V. Bipolar motor stimulation of the right
side of the spinal cord above the lesion did not
gave response even with 6V. Stimulation of the
left side of the spinal cord
was achieved with 1.7 V below the resected tumor
and 2V above the resected tumor.
Routine closure of the
wound. Before extubation another MRI
demonstrated radical resection of the tumor.
Smooth postoperative recovery.
The patient got some movement of the right foot
and the power of the left foot became slightly
better. She was sent to the ward.
MultiGen
Follow
Up
The patient came to the clinic 16-December-2018
walking with walker with full recovery of the
sensory deficit and full power of both lower
extremities except for slight weak dorsiflexion
right foot +4/5 with full control of urination
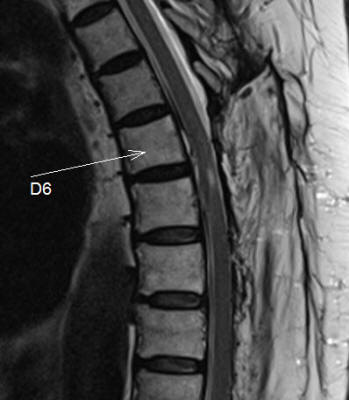
and defecation and was sent for control MRI
dorsal spine. See Fig-1 below.
Comments
The patient has huge meningioma with
pending complete paraplegia. Surgical removal is the only
solution.
This is the 138th case using the BPRF mode
with MultiGen. This procedure regained routine acceptance.
It became a usual part of the spine and peripheral nerves
surgery. Click here for
reference.
It could be that the spinal cord and
nerve is recovering minute by minute after decompression and
this can explain why the motor conductivity is improving. In
this case the left side was confirming that the left side of
the spinal cord was in good condition, but why the right
side of the spinal cord did not responded even to 6V above
the lesion was unclear. It could be a technical error.
Using the absence of the epidural fat as
guidance for severe compression, led us to the wrong
direction. The meningioma was causing hypertrophy of the
epidural fat with arterialized veins.
Intraoperative MRI is an integral
requirement for most cranial and spinal tumors surgery.
Without MRI, mistakes could happen even with long term
experience of the surgeon.
The slight improvement of the right lower
limb function is contradicted the stimulation parameters,
for what the surgeon must not trust the technology. In this
case it was misleading.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Inomed Riechert-Mundinger System, with three point
fixation is the most accurate system in the market. The microdrive and
its sensor gives feed back about the localization.
Inomed MER system
Leica HM500
The World's first and the only Head mounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
Fig-1: 2 years after total removal of the meningioma performed
17-December-2018 with almost full recovery of her neurologic status.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .