Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
23-JUNE-2014 MUHAMED THEEB AL-HORANI 85 YEARS
GLIOBLASTOMA MULTIFORME MIMICKING SOLITARY CA PROSTATE MTS TO THE LEFT TEMPORAL LOBE.
Anamnesis
The patient came to the clinic 18-June-2014
complaining of speech problems for 3 weeks and
headache left fronto-temporal for 10 days. The
patient was operated previously for discectomy
and underwent treatment for Ca prostate for 2
years. MRI brain done 14-June-2014 showing
rounded lesion left temporal lobe with ring
enhancement resembling MTS with massive
perifocal edema.
On examination; The patient is neurologically
free, except for the headache and difficult to
notice speech perception.
The patient was sent for cardio evaluation
and CXR was free.
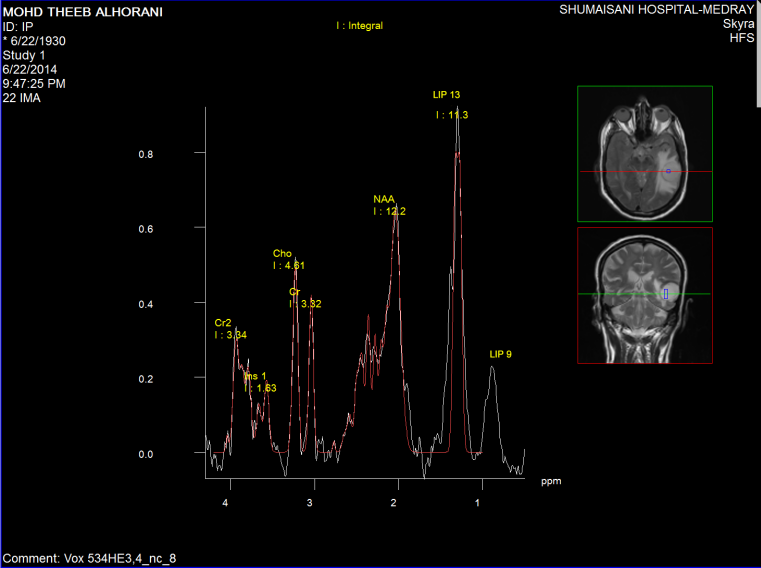
Spectroscopy was done the day before surgery,
supporting data for MTS (Figure1-6).
Osteoplastic craniotomy in the left temporal
area above the left ear with reflection of the
bone flap to the left ear. Cross-shape incision
of the dura. The tumor was seen directly with a
massive cluster of arterialized veins. Resection
of the tumor and part of it was sent for
histologic verification. There was no proper
cleavage to follow, instead the net of
arterialized veins, which were coagulated. The
wound was closed temporarily and intraoperative
MRI was done. It seems that the tumor was
resected, but some questionable remnant was
noted in the postero-superior of the resected
tumor cavity. The wound was inspected at that
area and the lesion had a look of normal brain,
but it was included in the resection. This part
was very near to Wernicke's area. The brain is
lax and strict hemostasis was achieved and
water-tight closure of the dura and routine
closure of the wound.
Smooth postoperative recovery.
The comprehension became more difficult after
surgery, but the patient has no other neurologic
deficit. The patient was sent to the ward.
The next postoperative day, the patient is
talking, walking, but understanding the verbal
command with difficulty.
Follow up
The final histologic result was high grade
glioma consistent with glioblastoma multiforme
with sections showing cellular tumor composing
of pleomorphic cells with high grade nuclear
atypia, giant tumor cells and brisk mitosis.
Gemistocytic cells were noted. Vascular
endothelial proliferation presented with
thrombosis. Necrosis is focal and minimal.
Fragments of brain tissue with gliosis was seen.
The neoplastic cells are GEAP +, PSA -, CK -. ( Dr. Fayez Hajjiri).
The patient was discharged 26-June-2014 with
speech comprehension difficulties.
Discussion
The glioblastoma multiforme, can mimic any tumor
morphologically, as appreciated by its name.
This case a demonstration, that it can mimic
even chemically other tumors including
metastasis. This spectroscopic picture was
typical for MTS, but the tumor turned to be
glioblastoma multiforme.
Comments
The patient under treatment for
adenocarcinoma of the prostate for 2 years. The lesion is
solitary and the chest is free.
Usually the MTS has good cleavage, but
this case had no cleavage. The pathologic arterialized veins
were seen all over the tumor clusters where as cluster of
rich leaves around this tumorous vascular tree.
In retrospective analysis, intraoperative
MRI must be performed with best protocol done before
surgery, where the tumor was best shown.
Concerning intraoperative functional MRI,
a new protocol of anaesthesia must be done, to achieve the
location of the functionally important areas such in this
case the area of Wernicke for speech comprehension.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
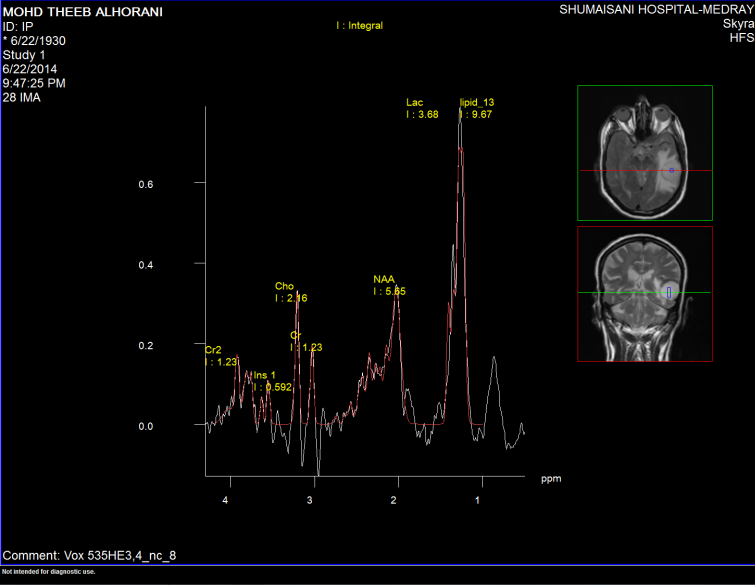
Figure-1: Short TE spectroscopy inside the mass showing
elevated LIP 13 and LIP 09 with slight elevation of Cho and NAA
suggesting the diagnosis of MTS more than glioblastoma
multiforme.
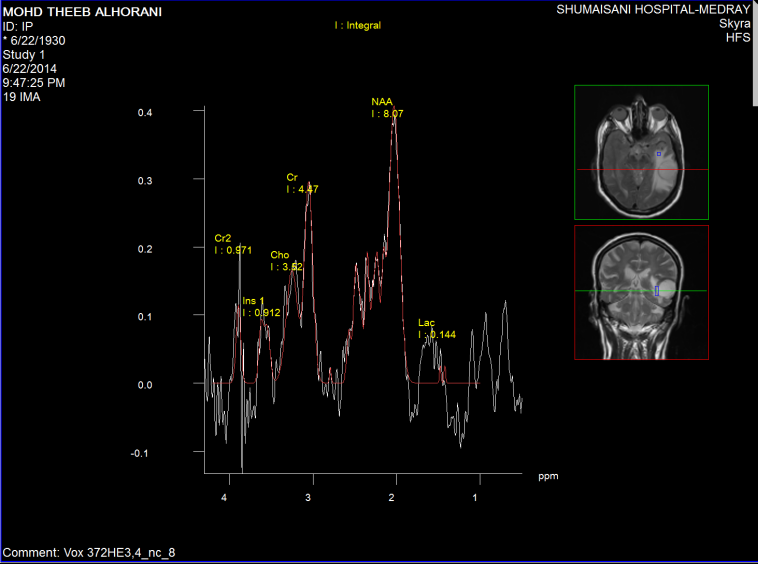
Figure-2: Short TE spectroscopy showing low Choline and high Cr and
NAA with low LIP 13 and 09 and low lactate, ruling out the
presence of malignant cloud around the tumor.
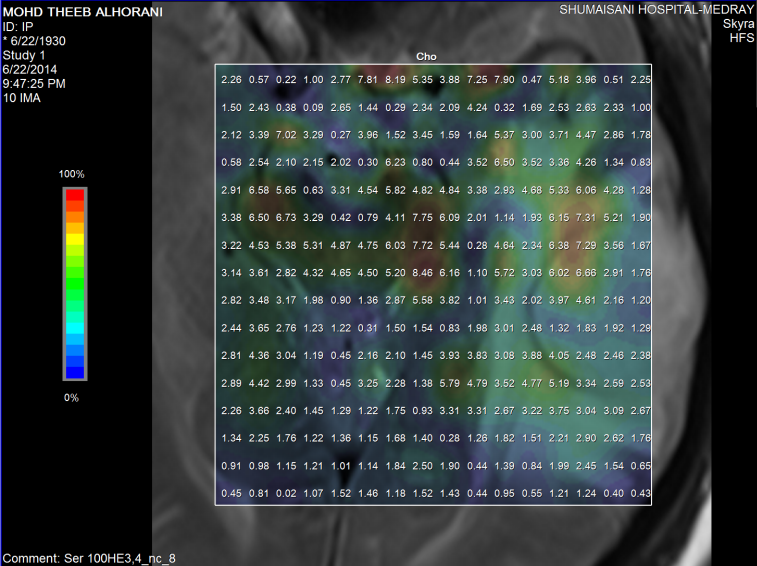
Fugure-3: Choline distribution using short TE 2D CS.
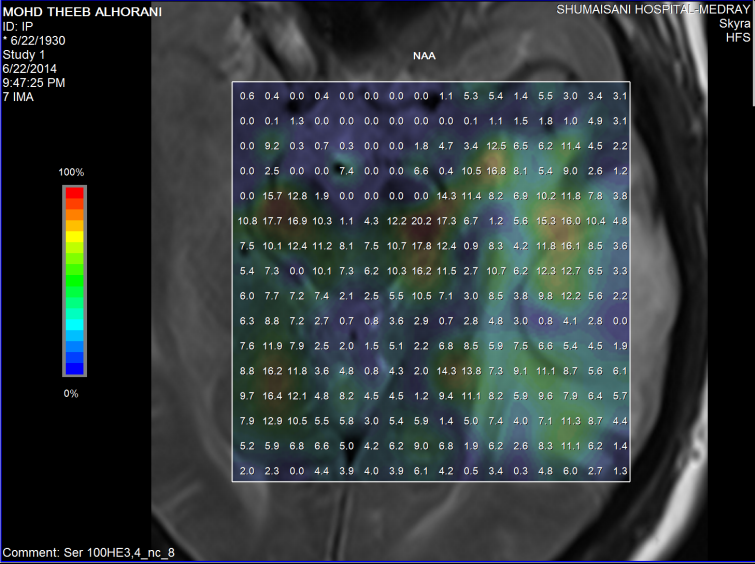
Figure-4: NAA distribution using short TE 2D CS.
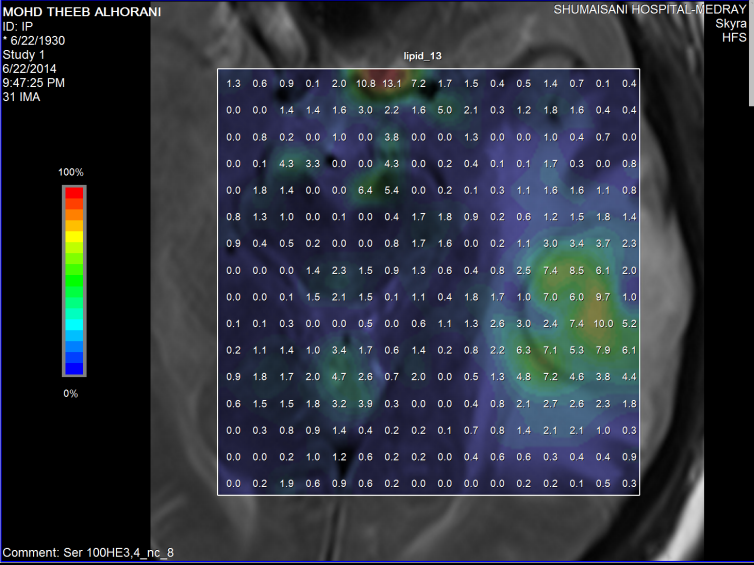
Figure-5: Elevated LIP 13 and LIP 09 inside the lesion using short
TE 2D CS.
Figure-6: Lipid 13 distribution using short TE 2D CS.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .