Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
24-DECEMBER-2009 MUHAMED SHAABAN AL-KHALILY 21
YEARS GIANT CONVEXITAL MENINGIOMA LEFT PARIETO-OCCIPITAL REGION.
Anamnesis:
The patient
was operated by me 22-January-2004 for
huge meningioma of the dorsal spine at D6
right side. The patient was neurologically free
after the operation and the last MRI of the
dorsal spine was free performed 21-June-2008
with mild kyphosis at this level.
The patient then came to the
clinic 20-December-2009 complaining of headache
for 2 months in the left occipital region. The
headache was progressive with nausea and
awakening him during night. The last 2 days he
progressed atonic attacks .
MRI brain done
10-December-2009 showing giant convexital
meningioma in the left occipito-parietal region.
On examination: the patient
is neurologically free.
Osteoplastic wide craniotomy
of the left occipito-parietal region. The bone
flap was involved with the tumor, for what it
was removed and sent for boiling in 125 degrees
Celsius for 15 min in the autoclave. The tumor
had very wide matrix and the healthy dura was
incised parallel to the edge of the tumorous
dura. The tumor was rich in vascularity and it
was coagulated and debulked. The tumor was sent
for fresh frozen section, which confirmed
meningiomatous nature of the tumor. The cleavage
between the tumor and the surrounding brain was
identified and sharp dissection was proceeded
until the tumor was radically removed. All the
running veins and arterioles were respected and
preserved until the end of resection.
After meticulous heamostasis,
BloodSTOP ix was
used several times and it was found that it was
a bad option, because it seems it trigger
bleeding and it was impossible to be sure what
is going on under its layer. It even
triggered arterial bleeding, for what it was
washed out and another trail was performed to
see what is going on. The same disadvantages
repeated and the material was cleaned and
surgicel was applied in the tumor bed, which
showed good control and dry field.
Lyodura was replaced of the
removed tumorous dura and water-tight closure
was achieved. The treated bone flap was returned
to its place and fixed with 9 points. Routine
closure of the wound with Ready-Vac inserted
under the scalp.
The patient was extubated and
sent to the ICU without any neurological
deficit.
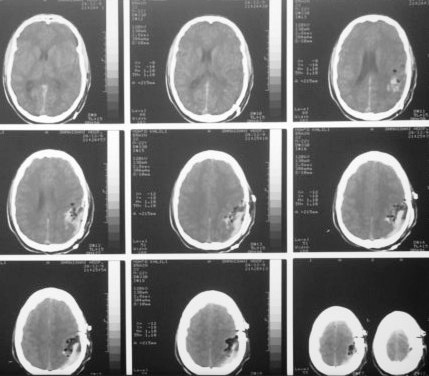
Control CT-scan 6 hour after
surgery.
Comments
BloodSTOP ix is a bad
option for such a surgery and it seems it
triggers bleeding even from previously
controlled sites. It has many disadvantages,
that it is better to avoid using this material.
Surgicel is more superior and lacking of such
disadvantages.
Even the tumor was of giant
size, the patient was neurologically free before
and after the surgery.
The patient has
meningiomatosis, for what he was operated 5
years ago for spinal meningioma and now for
supratentorial meningioma.
Please! wait for 3-5 min till the
video start to load. It depends upon the internet
connection.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .