Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
21-MAY-2017 MUNIF MLEHAN AL-SHAMARI 40 YEARS
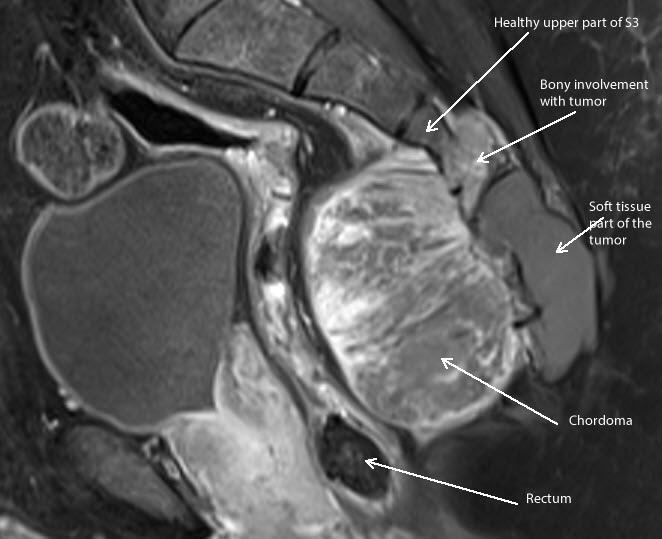
HUGE CHORDOMA WITH DESTRUCTION OF THE LOWER SACROCOCCYGEAL REGION BELOW THE LEFT
S2 ROOT WITH EXTRA AND INTRAPELVIC EXPANSION.
Anamnesis
The patient came to the clinic 15-May-2017 complaining of
left sciatica for 3 months. The patient was
operated for "anal fissure" 6 months ago without
improvement. MRI bad quality done
06-December-2016 showing chordoma at the lower
half of the sacrum. Biopsy was done, confirmed
chordoma nature of the lesion. The patient has
difficult micturition the last 2 months.
On examination, the patient is limping with
exaggerated scoliotic stance. SLRS
was 40 degrees with pain in left side. There is weak
dorsi and planterflexion left foot -4/5, and
weak adduction of the knee 4/5. There is
analgesia in the left perianal region with weak
sphincter ani left side.
The patient was sent for investigations and
neuro MRI of the pelvis with TWIST and
spectroscopy of the lesion was performed showing
complete destruction of the coccygeum and left
side of the sacral bone up to the emergence of
the left S2 root. The SIJs are anatomically
preserved. The rectum is pushed anterior without
involvement. No arterial feeders were noted. The
left S2,3,4 are involved in the mass. The mass
is growing behind the sacrococcygeal structures
under the skin and fulfilling the pelvic cavity.
Spectroscopy of the mass showed moderate
elevation of Choline, NAA, lipid 1.3 and 0.9
ppm.
Skeletonization of the
sacrococcygeal area. The tumor is destroying the S3
down to the coccygeum more the left side. Step wise
resection was performed until the rectum was seen
and the left S3 and S2 were preserved and the motor
response was adequate. The tumor is highly
vascularised that the patient was in need for 4
units of blood and 2 units FFP. The resected tumor
was sent for histologic study. Check MRI showed that
there is huge fragment in the right lower pole. This
part was resected with the tumorous coccygeum. Parts
of the tumor were severely adherent to the rectum,
that it was impossible to remove them without
violating the posterior wall of the rectum.
Coagulation of these fragments and another check MRI
was performed and these parts were seen. Routine
closure of the wound.
Smooth postoperative recovery. The power of
the left normalized and he was sciatica free.
He was sent to the ward.
MultiGen
Follow
Up
The final histologic result was low-grade myxoid
chondrosarcoma with CD99 and Vimentin
positive and negative for S100 and E-Cadherin.
Comments
The patient has several problems, which
require surgical correction, stenosis at 2 levels and
spondylolisthesis.
This is the 118th case using the MultiGen. This procedure regained routine acceptance.
It became a usual part of the spine and peripheral nerves
surgery. Click here for
reference.
It is better not to perforate the rectum
by leaving 5% of the mass, since it is benign. Time will
tell the speed of the recurrence.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Inomed Riechert-Mundinger System, with three point
fixation is the most accurate system in the market. The microdrive and
its sensor gives feed back about the localization.
Inomed MER system
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
CT-scan with 3D reconstruction showing the deformed bone reaching
the left S2 root.
Anterior aspect of the bony structures modeled and cut for better
vision using ORS Visual software.
Midsagittal part showing the tumor relationship.
Spectroscopy showing the components of the tumor.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .