Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
24-OCTOBER-2011 RASHED ALI RADWAN 20 YEARS
DIRECT INJURY TO THE RIGHT BRACHIAL PLEXUS AT NERVE LEVEL.
Anamnesis
The
patient came to the clinic 22-October-2011
complaining of complete non-function of the
right radial, ulnar and median nerves after cut
wound right brachial brachial plexus through the
deltoid muscle and proposed graft of the alleged
cut subclavian artery 30-August-2011.
The
patient performed 2 EMG with EC studies the last
19-October-2011 confirming that the mentioned
nerves are completely non-functioning.
On
examination: the right MCN is completely normal.
The right axillary nerve also normal. The
radial, ulnar and median are completely silent.
There is severe causalgia when touching the
right hand.
The old
approach was refreshed and extended down to
expose the ulnar and median nerves below the
lesion. There is massive scar and neurolysis was
performed with difficulty , especially the median
which was buried in an arterial net , which is
the graft which was harvested from the right
femoral area. It was above the median nerve and
was draining to various venous channels
superior. The wound was extended superiorly to
expose the cords and the subclavian artery. The
posterior, lateral and medial cords were
identified and also their branches and studying
them with ISIS High-Line using the brachial
plexus set, it was possible to see that the
axillary, MCN and the triceps muscle are
responding well after their neurolysis. The
artery was normal at this level.
Continuing dissection down and up and from all
directions, it became clear, that the subclavian
artery is not torn and the graft was stitched to
one of its branches, going superiorly engulfing
the nerves and draining to the veins. The artery
was inspected form the most proximal down to the
most distal part. It is functioning well and
there is no graft between them. The arterialized
venous graft was dissected off and coagulated to
prevent it from harming the nerves. All the
running nerves were looking healthy and there is
no ganglion, nor atrophy or disconnection.
Several time revision was performed to ensure
that there is no missing data. The retrograde
stimulation of the right median nerve took place
at the end of the operation, that it could
elicit the right MCN.
Routine
closure of the wound. Smooth postoperative
recovery.
Follow Up
The patient came 26-June-2012 with signs of full
recovery of the MCN. radial nerves. The patient
can dorsiflex the wrist, but has minimal
dorsiflexion of the fingers due to spastic
pattern. The brachioradialis muscle is 5/5. All
the proximal muscles of the forearm are
functioning, which means that, despite the
severe damage of the median and ulnar nerves,
but they start to recover. The patient was
advised to continue more aggressive
physiotherapy to prevent contracture of the MPJs
of the hands.
Please! wait for 3-5 min till the
video start to load. It depends upon the internet
connection.
Comments
The patient got stab wound injury to the right
brachial plexus. The graft of the cut subclavian
artery misled the speculation and the proper
planning for surgery. The artery and running
nerves were not cut. It is mostly that the
arterialized venous graft was playing a negative
role in the recovery process of the nerves.
Neurolysis and elimination of the arterialized
venous fistula which was engulfing all the
nerves is mandatory in this case.
It became retrospectively clear, why the patient
was complaining of causalgia. It is due to
arterial engulfment of the nerves running at the
involved site.
It took me 5 hours to understand that the
subclavian artery was not grafted and the graft
was between one of the small distal branches of
the brachial artery and one of the veins
proximally.
Such a case is not reported in the literature to
my knowledge.
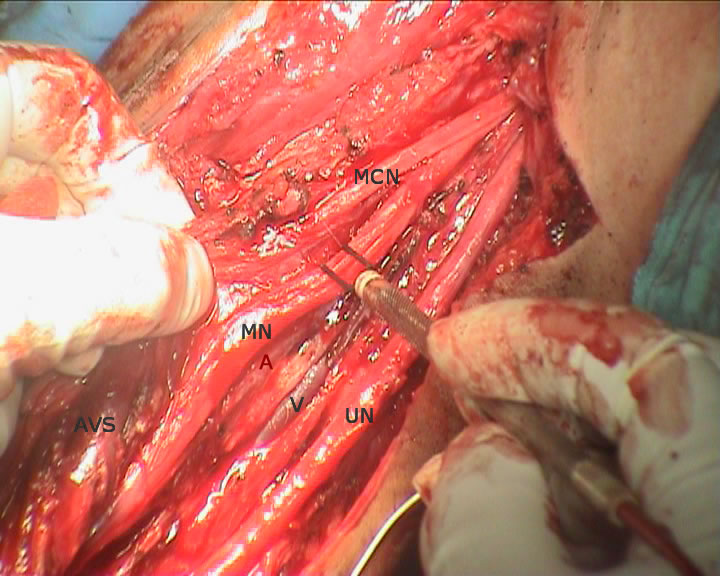
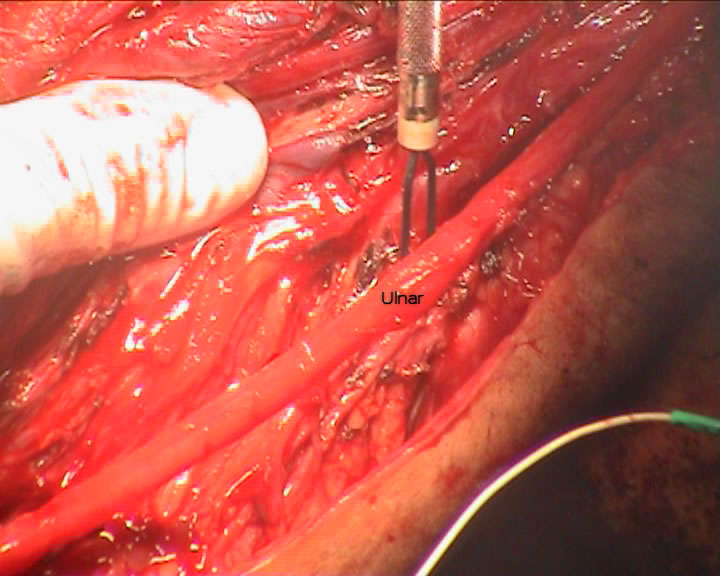
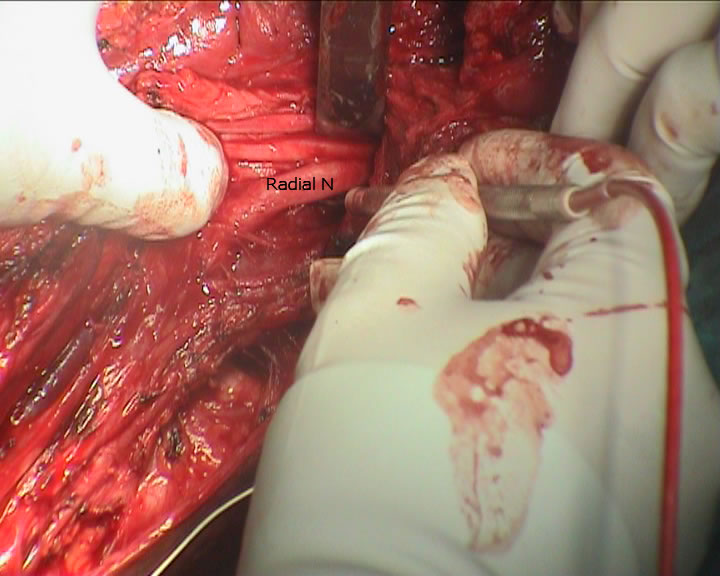
Pictures during surgery showing the major nerves with intact
morphological structure, but variable functional status.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .