Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
21-MAY-2025 SAMIR SALEM DABABNEH 68 YEARS
TETRAPARESIS AFTER POSTERIOR CERVICAL DECOMPRESSION WITH SPONDYLOLISTHESIS C4-5
AND C5-6.
Anamnesis
The patient came to the clinic 04-Januay-2025
telling that he deteriorated dramatically with
subsequent tetraparesis after performed
posterior cervical decompression of C3-4-5-6
elsewhere 14-November-2024.
On examination, the patient has shuffling gait. Can walk with
difficulty, cannot be
evaluated for Romberg stance. There is pain when
turning the head downward, There is analgesia of the right
hand. Hoffman positive more brisk in the
left side and the deep tendon reflexes
exaggerated in the left upper limb. There is
weak grip right hand 4/5 and extension both hands
3/5 with both triceps muscle 2/5. SLRS was 10
degrees right side and 40 degrees left side
without pain. There is weak right iliopsoas
muscle, right quadriceps 3/5 and dorsiflexion
right foot 4/5. Knee jerk exaggerated both
sides, but Babinski and clonus negative both
legs. Normal defecation and micturition.
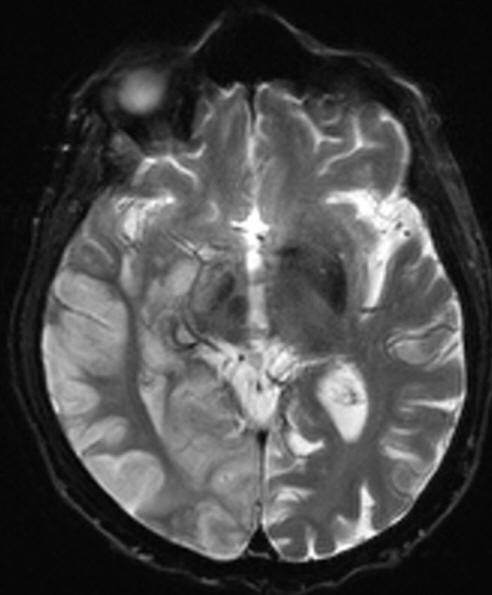
The patient was sent for investigations
and MRI brain done
20-February-2025 showing scattered infarction
both cerebral hemispheres and malacia of
the spinal cord more at C5-6. Dynamic
studies showed spondylolisthesis C4-5 and C5-6
with the body of C5 pushed posterior. Medical
treatment was started but the patient telling
that is condition is deteriorating and asking
for fixating his flail spine. The patient was
asked to stop all anticoagulant elements and to
be seen by cardiologist.
Using the C-arm, the level of
C4-5-6 was identified and surgical exposure of C4-5-6 was achieved.
Using Nuvasive Helix cervical plate 38 mm and 4
variable angle screws 4.0x 15 mm o C4 and C6 and
2 screws fixed angle 4.0x 15 mm to C5, fusion of
C4-5-6 was achieved. Routine closure of the
wound. The patient was sent to the ward.
Clinically he was the same.
Nuvasive Helix cervical plate.
FOLLOW UP
The patient shows improvement, but he has no
accompanying relative and and when I visited his
at 7.00 p.m. the patient was in the ground and a
lot of blood due to disconnected cannula, for
what I called the medical personnel to wash him
and the room and the bed. Hiss brother a 85
years age was told and I toled the medical staff
to keep close eye upon him.
The next day morning when I visited him, no
accompanying relatives and the patient is in the
ground with huge bruise in the left frontal area
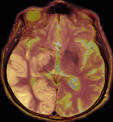
and with left sided hemiplegia. Urgent CT-scan
was done to rule out intracranial hematoma.
Contra coup contusion with good
arterial circulation.
The patient then sent to the ICU to have more
strict observation.
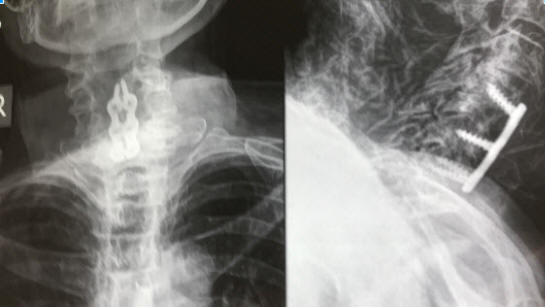
Check cervical X-ray done 25-May-2025
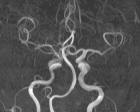
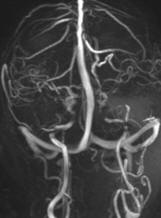
MRI with MRA, MRV and TWIST confirming the patency of
the right ICA. The protocol done 29-May-2025 the day
before discharge.
Comments
The patient has malacia of the spinal
cord due to previous cervical spinal canal stenosis and
deterioration took place after surgery. Dynamic studies were
not performed before the first surgery. The flail C5 further
took place after surgery, which led to more further
deterioration. At least fixation of the segment can prevent
this element of instability.
Usually the problem with many visitors,
but it is the fist time in my life I did not realized that
no accompanying relatives. In the future I must pay
attention to this situation and take the appropriate
measures to avoid such unexpected postoperative unlucky
scenarios.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Inomed Riechert-Mundinger System, with three point
fixation is the most accurate system in the market. The microdrive and
its sensor gives feed back about the localization.
Inomed MER system
Leica HM500
The World's first and the only Head mounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
LooksCam II Xenosys in the run starting from 14-March-2021 with
SheerVision TTL x4 magnification.
Cios-Spin flat panel in the run.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .