Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
09-FEBRUARY-2014 SAMIRA FAZEH ABU-DARWEESH 49
YEARS LEFT CPA GIANT MENINGIOMA.
Anamnesis
The patient came to the clinic 03-February-2014
complaining of left sided headache for 28 years
and considered as having migraine with
exacerbation the last month. MRI of the brain of
bad quality done at Al-Bashir hospital
12-October-2011 reported to be normal, but there
was a lesion in the left CPA. The last month has
ataxic gait. Numbness of the left side of the
face and the the tongue. The patient is left
handed. Sialorrhea from the left side.
On examination; the patient is alert is
responding to all verbal responses. She has
hypalgesia of the left side of the face. Romberg
stable. The hearing decreased in the left side
with tinnitus left ear for 4-5 months. There is
weak right upper and lower limbs right side 4/5.
Hoffmann was positive in the right. Babinski and
clonus of the right foot ?.
The patient sent for new MRI of the brain with
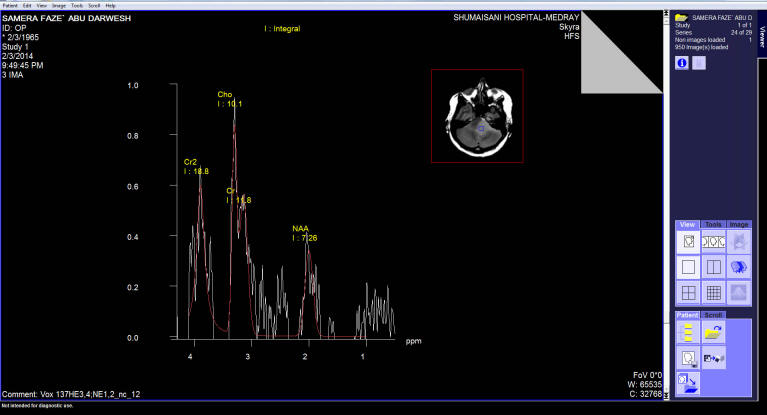
contrast and spectroscopy. All data were in
favor of huge left CPA meningioma 33x32x30 mm
dimension. MRA showed compression of the basilar
artery with the corresponding PICA by the tumor
mass. Spectroscopy was typical of meningioma.
Setting position. Craniotomy done to expose the
left cerebellar hemisphere and the left
transverse sinus and abutting the left sigmoid
sinus. The dura was opened to reach the
subtentorial area. The meningioma was seen at
the most anterior parts. The tentorium was not
involved by the matrix of the tumor, nor the
superior petrosal sinus. The tumor was rubbery
in consistency with good cleavage. Piece meal
resection was started and the tumor was
dissected off the brain stem, cerebellar
hemisphere. After total resection of the tumor,
the trigeminal nerve was pushed upward flattened
and stuck with the brainstem. The facial and
vestibulo-cochlear nerves were pushed down and
posterior. The left AICA and its branches were
preserved. The tumor matrix was superior to the
meatus acousticus internus. Some feeders were
coagulated to achieve Hemostasis. Further
hemostasis was achieved by applying surgicele.
The patient was sent to MRI to confirm the total
resection of the tumor. There is no any residual
mass, except the surgicele. The patient now in
supine position and routine closure of the
wound.
Smooth postoperative
recovery. The facial and all the nerves of the
area are functioning properly. Sent to the ICU.
Postoperative
course:
The patient complained of double vision when
looking to the left. It could be explained by
the reaction of the quadrigeminal structures
after tumor removal.
The final histologic result was fibroblastic
meningioma.
Comments
The patient underwent intraoperative MRI to
confirm the radical resection of the tumor. The
good shape of the brainstem, gave the decision,
that the patient can be extubated immediately
after surgery and this was achieved.
The essential purpose of intraoperative MRI
control is to catch any complication during
surgery and to know exactly what happened and to
respond accordingly.
The patient was operated in setting position
during tumor removal, but the surgery was
continued after MRI control in supine position.
A massive bleeding took place from the
intraoseous veins from the bone defect. The
conclusion is that it is mandatory to wax all
the bone edges for 2 reasons. First the prevent
the progression of air embolism, second: to
prevent postoperative extradural bleeding.
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
Spectroscopy done before surgery confirming the
meningioma charcter of the tumor.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .