Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
29-JANUARY-2015 TURKEY KHALAF MUHAMMED 4 YEARS HUGE
MEDULLOBLASTOMA WITH EXTENSION TO BOTH FORAMINA OF LEUSCHKO.
Anamnesis
The patient came to the clinic with his parents
27-January-2015 complaining of vomiting and
drowsiness for 1 month with the last weak
complaining of diffuse headache. CT-scan done
25-January-2015, showing a midline posterior
fossa mass.
On examination, Considering his age, it was
difficult to evaluate him for Romberg
positioning, but there was no nystagmus and
neurologically was free.
The patient was admitted urgently to the
hospital and MRI of the brain with contrast with
MRA of the brain and carotids with spectroscopy
and DTI were performed under G.A. There is huge
medulloblastoma vermian localization with
extension to both foramina of Leuschko. So as to
avoid putting shunt to him, massive doses of
Decadron were started and the patient started to
improve.
Midline posterior occipital approach in setting
position. The bone flap reflected to the neck
inferior. The dura was opened in V-shape
fashion. The tonsils were shifted downward and
the vermis is prominent by the tumor. Sharp
dissection of the inferior pole of the vermis (
The uvula). The tumor was highly vascular with
rich blood supply. The tumor was coagulated
sucked and most of the upper part was removed.
The inferior part was was removed until the
obex with related structures were seen. The left
part of the tumor was followed and resected
until the foramen of Leuschko was seen and the
left inferior cerebellar peduncle was preserved.
The same maneuver was undertaken in the right
side. The tumor inside the 4th ventricle was
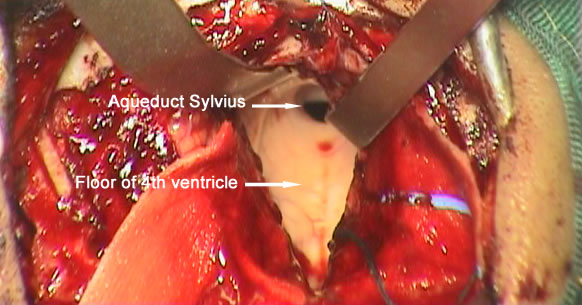
removed and the floor of the 4th ventricle was
seen intact with widened aqueduct through which
the third ventricle was seen. The superior
medullary velum was respected. The floor of the
4th ventricle was flattened due to the previous
compression effect of the tumor, that it was
impossible to see the median sulcus, nor the
paramedian sulci limitantes or the hypoglossal
trigone elevations at the calamis scriptorius. I
got the impression that the tumor was totally
resected, for what intraoperative MRI control
with contrast was done. There is still part of
the tumor in the right upper corner and the
right foramen of Leuschko. Resection of this
part was achieved until the normal cerebellar
tissues were seen at these angles. Strict
hemostasis with water-tight closure of the dura
and bone flap was secured with 2 stitches and
routine closure of the wound.
Smooth postoperative recovery.
The patient extubated and sent to the ICU for 24
hours observation.
Comments
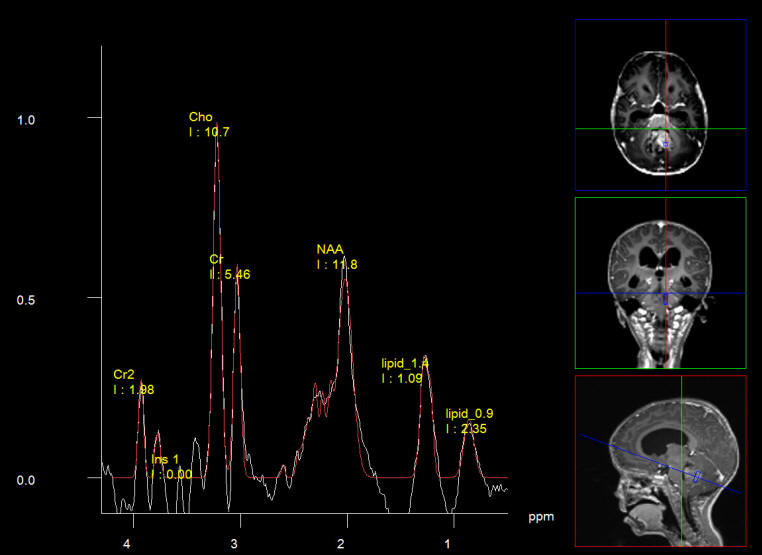
The patient has typical spectroscopic
data supporting medulloblastoma. The histologic result will
give the answer.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
Inomed MER system
Spectroscopy showing typical data for medulloblastoma
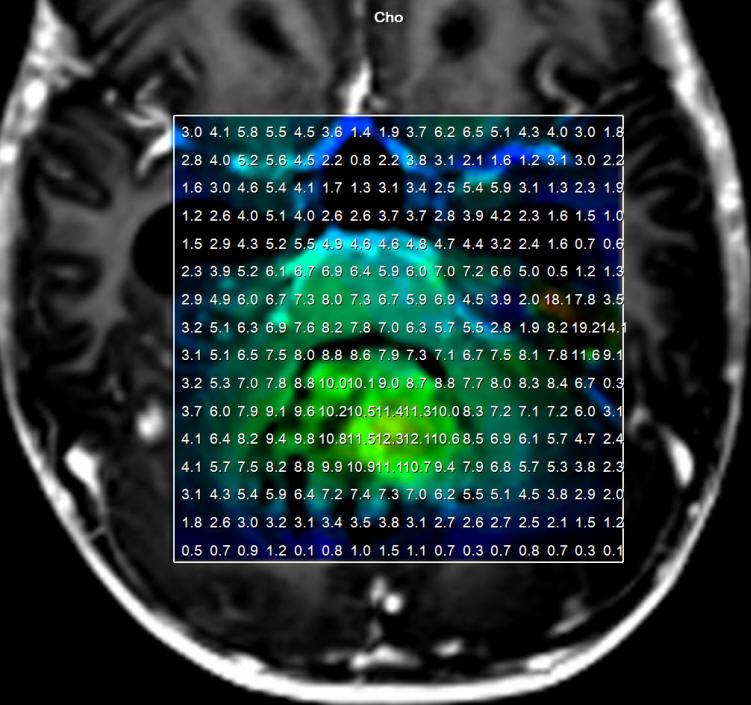
Choline distribution in the medulloblastoma.
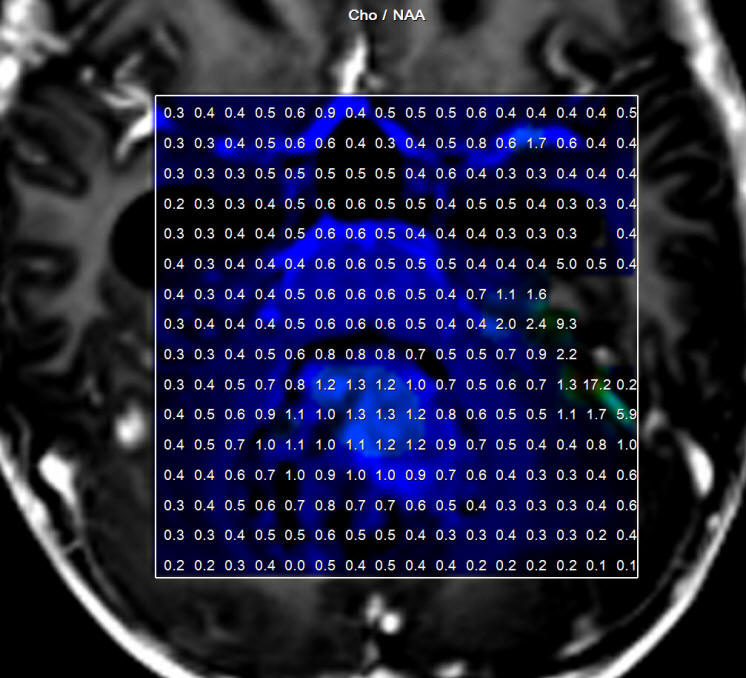
Cho/NAA ration distribution of the medulloblastoma.
Floor of the 4th ventricle after removal of the medulloblastoma.
MRI done during surgery showing the missing part of the tumor, which
was subsequently removed.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .