Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
24-OCTOBER-2012
WAHID AHMAD CUTNA 54 YEARS THROMBOSIS OF THE LEFT ICA AFTER
ENDARTERECTOMY 2 DAYS AGO.
Anamnesis
The patient was operated by me
21-October-2012 for complete stenosis left
ICA. The patient was sent the the ICU and doing
OK. After 12 hours, he showed deterioration of
his right sided paresis till deep paresis of the
right upper limb with the right side of the face
with speech difficulty. The heparinization
protocol was intensified and repeat CT-scans did
not show any changes. CT-angio done showing
occlusion of the left ICA.
The wound was opened and the
ICA dissection was extended superior. The ICA is
pulsating, but weaker than the ECA and CCA. The
Javid shunt was occluded from its long side
and the shorter side was inserted to the ICA
above the graft through a vertical incision
around 10 mm. The flow from the grafted side was
excellent, but from the cranial side was zero.
Angiography was done showing good filling of the
left MCA and ACA. The balloon was inflated and
withdrawn with the thrombus and debris
outside the artery. The same procedure was done
with the log end of the Javid shunt. No more
thrombi. The flow was excellent from above and
angiography repeated another time to show good
filling of the left MCA and ACA and most of the
ICA. The arterial defect was closed using 5 zero
nylon suture.
Routine closure of the wound. Smooth
postoperative recovery with same neurologic
deficit as before the second surgery.
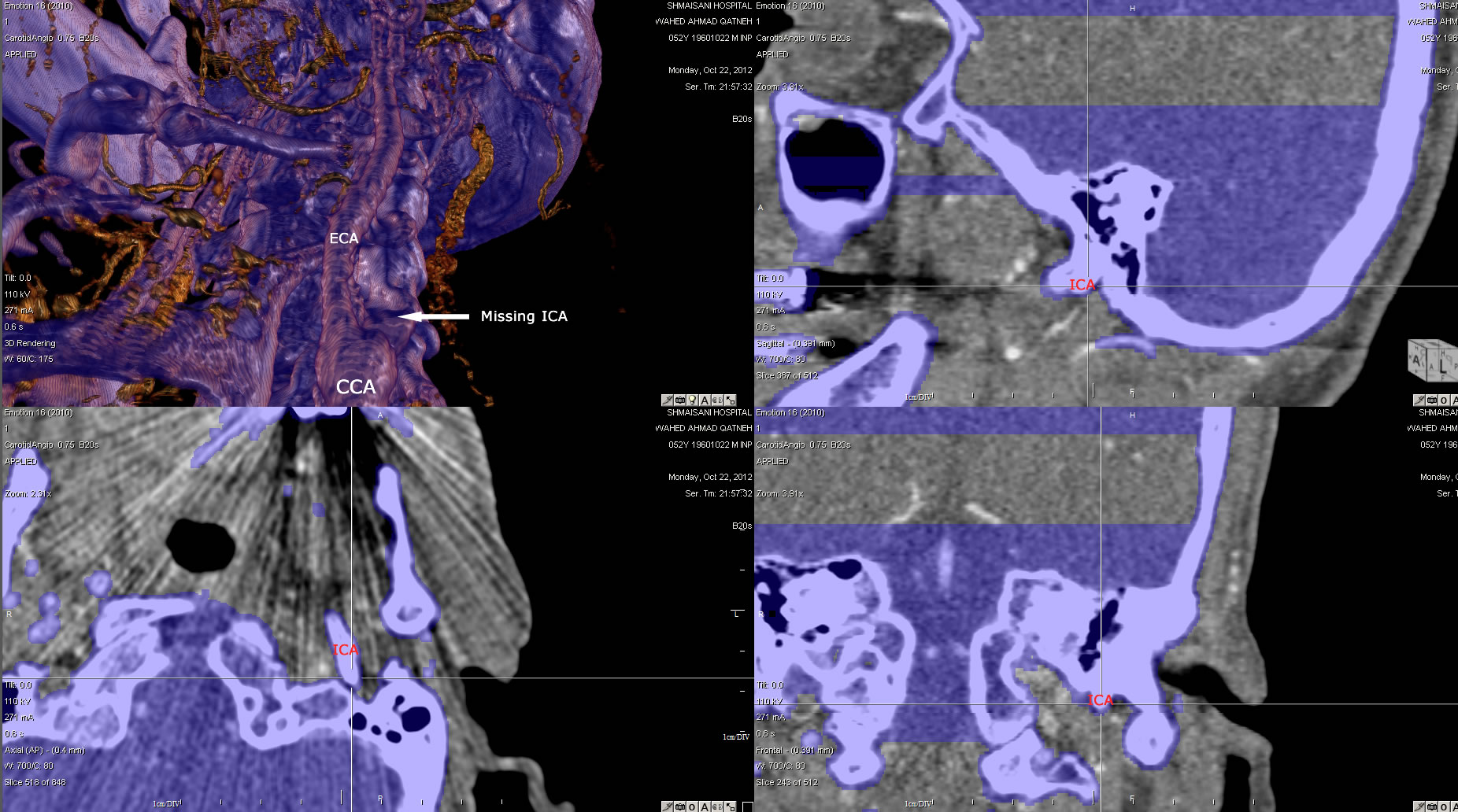
CT-angio performed before surgery
showing thrombosis of the left ICA
Please! wait for 3-5 min till the
video start to load. It depends upon the internet
connection.
Comments
The patient progressed
thrombosis above the grafted area several hours
after surgery. Opening the wound and meticulous
cleaning of the thrombus is the best option.
Misreading of the ORSVisual and other programs showing
in the left upper case absence of the left ICA but in
the others presence of the carotid even in the area
abutting the foramen caroticum. This confusion led us to
explore the operative site and perform the above
mentioned procedure. Angiography remains the gold
standard , and inspection of the wound and removal of
this tiny clot with tiny debris was necessary to resolve
such confusion.
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .