![]()
Glomus jugulare tumors are among the most difficult tumors arising in the base of the skull and considered the most challenging for surgical treatment, since the patients usually come to surgery in advanced state, after failure of adjunctive treatment such as embolization, radiotherapy or previous attempts for partial resection. The neurological state of the patients was usually with involvement of the caudal group of nerves and even with infiltrative destruction of the facial nerve in several cases.
During the period of 1980-2004 I had the experience with 10 cases of what could be considered by Ugo Fisch & Douglas Mattox as class C4De2Di2 tumors. For the academic pools and data concerning these tumors you can follow the references. Here, the main concentration is directed to the personal experience of difficulties during operative and the postoperative period. One case was mentioned in the article: AVOIDANCE OF COSMETIC DEFORMITY IN APPROACHING THE PETROCLIVAL REGION DURING COMBINED TRANSPETROSAL APPROACH.
Case Presentation:
A young married women 27 years age came to the clinic 30-04-2003, complaining of severe headache for more than 3 years duration with hearing loss in the left ear for more than 2 years, ataxia for 11 months, swallowing difficulty for 9 months and complete left facial paralysis of peripheral type for 4 months with right sided hemiparesis and hypalgesia. MRI performed 22-07-2001 showed a mass in the left jugular bulb extending to the sigmoid and transverse sinuses left side. Attempt for embolization caused visual field scatomas . MRI done 12-01-2003 showed enlargement of the tumor four times in volume. The patient on examination, beside the above mentioned complains showed severe atrophy of the left side of the tongue with uvula sagging to the right in gag reflex. It was impossible to perform Romberg test due to inability of the patient to stand. Slight paresis of the left abducens nerve was noted and the voice was dysphonic.
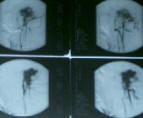
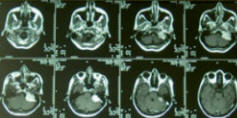
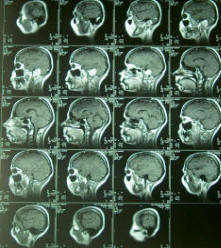
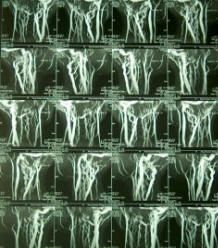
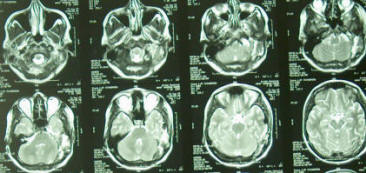
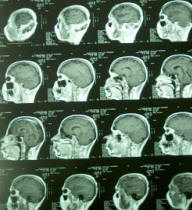
Preoperative angiogram and MRI showing the glomus jugulare tumor shifting the brain stem and totally destroying the left middle and inner ear structures.
| VIDEO RECORDING OF THE CASE | |
The patient was admitted to Al-Shmaisani hospital in Amman - Jordan and operated 17-05-2003. Using the modified trasotic translabyrinthine approach with preservation of the mastoid shell as described elsewhere, it was possible to track the facial nerve, which seemed to be completely destroyed by the tumor. The inferior margin of the approach was extended to expose the IJV, which was checked for patency. It turned to be completely occluded and after its ligation below the involved mass, it was opened. resection of that part was achieved. The facial nerve at its emergence from the brainstem was anastomosed using sural nerve to the postfallopian part. To achieve good alignment of the proximal part , 2 hours spent to put three 10 zero nylon stitches. Using artificial tubes , was impossible due to insufficient length of the proximal part. The dura was closed leaving intentionally small defect to the anastomosis, to avoid mechanical pressure and the defect was glued by small piece of muscle. A muscle was harvested from the lower abdomen with fat to fill the spaces under the bone flap , which was reflected back and closed. The operation took more than 20 hours and the patient required 16 units of blood and 12 units of FFP. Postoperative period was surprisingly unremarkable and she was not in need for tracheostomy, which was highly suspected. NGT feeding was continued for 2 weeks, due to deterioration of the caudal group of nerves , as usual and the left abducens nerve became completely paralyzed after the operation, despite the fact, that it was not touched or violated during surgery.
| |
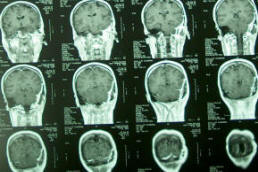 |  | 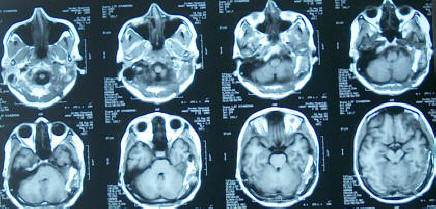 |
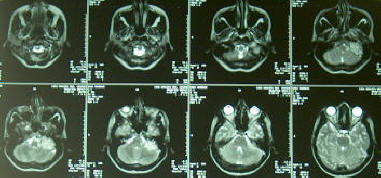
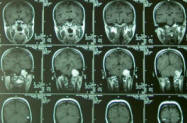
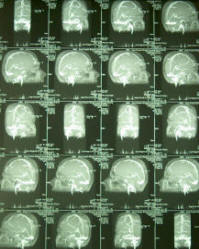
 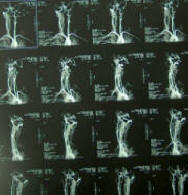 MRI, MRA, MRV of the patient performed 28-07-2003 demonstrating the radical resection of the tumor and bone flap holding the muscle harvested from the quadriceps muscle | ||
The patient was seen several times at ambulatory first with stitch sinus and the left abducens was completely paralyzed. The patient then slowly, but steadily showed marked recovery of her hemiparesis , hypalgesia and the left trapezius became more stronger . The abducens became fully functional after four months. The atrophy of the left side of the tongue regressed and the swallowing and speech dramatically improved. After 9 months the facial nerve start to show dramatic signs of recovery. The patient came 12-12-2004 with almost complete recovery of her facial nerve function.
Discussion:
Conclusions:
References:
Jon H. Robertson, M.D., Jason A. Brodkey, M.D. Glomus Jugulare Tumors. The Practice of Neurosurgery. GeorgeT. Tindall, Paul R. Cooper & Daniel L. Barrow. Volume 1. 67: 1005-1020.
Ugo Fisch & Douglas Mattox: Classification of Glomus Temporale Tumors in Microsurgery of the Skull Base . Thieme 149-153.
The author have made every effort to trace the copyright holders for borrowed material. If inadvertently overlooked any, will be pleased to make the necessary arrangements at the first opportunity.
![]()