Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
20-MAY-2014
ISHAQ MUHAMED GHNEMAT 60 YEARS EARLY RECURRENCE OF RIGHT TRIGEMINAL NEURALGIA.
Anamnesis
The patient was operated by me
18-May-2014 for trigeminal neuralgia. The
patient was complicated by dense left sided
plegia which resolved over hours and the
neuralgia disappeared. But the evening of
19-May-2014 the patient started to complain of
neuralgia attacks and started to escalate over
the next hours, that the mid day of today, the
neuralgia became intolerable.
On examination; the patient has paresis of the
left side of the body. The facial and vestibular
nerves are intact.
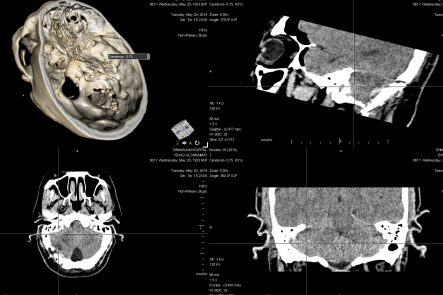
CT-scan was done before surgery to see the
craniotomy site and the the presence of possible
hematoma or huge infarctions. There was an
infarction of the right cerebellar pole, without
any shift to major structures.
The patient was taken to the operating theater
at 8.00 p.m. and put in the setting position.
The dura was opened and the lacerated cerebellar
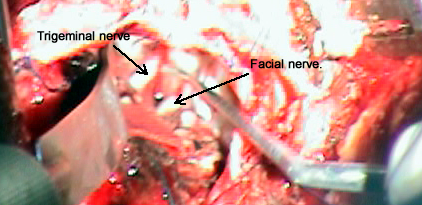
pole was sucked out. The facial nerve was
inspected to preserve it. The trigeminal nerve
was seen and the Gelfoam was found and removed.
The Teflon piece was not found. It mostly
slipped due to infarction to unknown place. The
left at first surgery arachnoid 90 degrees
of the 360 degrees was dissected off. The origin
of the trigeminal nerve was circumferentially
inspected and all the running in the surround
veins were coagulated. The arterial loops were
missing in the area and this was mostly due the
severe spasm. A piece of muscle was taken and
the trigeminal nerve was engulfed
circumferentially and the edges of the muscle
were attached with 2 titanium liga clips.
Smooth postoperative recovery.
The neuralgia disappeared and the paresis is
still the same as before the second surgery. The
patient sent to the ICU.
The CT-scan done before surgery showing the infarction
and the Teflon patch is missing.
The trigeminal and facial nerves are seen in the
operative field.
Comments
This case was complicated with
severe spasm, which led to cerebellar infarction, which led
to slippage of the Teflon patch and recurrence of the
trigeminal neuralgia.
For more information about trigeminal
neuralgia and MVD click
here and here!
The second surgery was for 2 reasons:
Lacerotomy will speed the recovery of the infarction and
elimination of the trigeminal neuralgia.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .