Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
18-DECEMBER-2014 SHAIMA FALAH HASAN 29 YEARS
TB PACHYMENINGITIS WITH SECONDARY FLARE WITH COMPLETE PARAPLEGIA.
Anamnesis
The patient was operated by me
10-December-2014 for tb pachymeningitis and
showed signs of improvement. She came
12-June-2014 walking with aid with slight
diffuse weak both lower limbs with power ranging
from 5/5 -4/5.with scattered hypalgesia below
the umbilicus with preserved sensation of the
left leg below the knee. The patient then came to the clinic 17-December-2014
complaining of complete paraplegia the last day
with Foley catheter in wheelchair. She
started to dyseasthesia of the left flank 2
months ago which gradually spread to both sides.
20 days ago she got sudden onset loss of
sensation of the right leg. The last 3 days got
progressing paraplegia with the last movement
was noted yesterday of the toes of the left
foot.
On examination, the patient has complete
paraplegia and analgesia 7 cm above the
umbilicus.
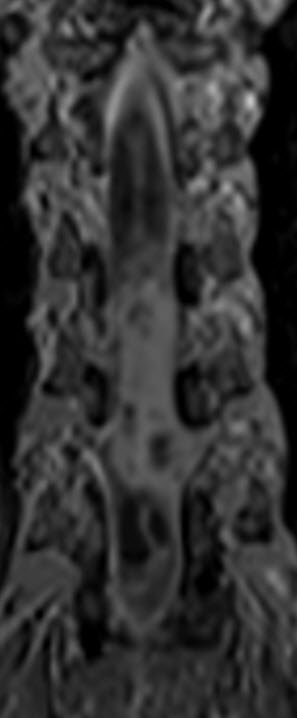
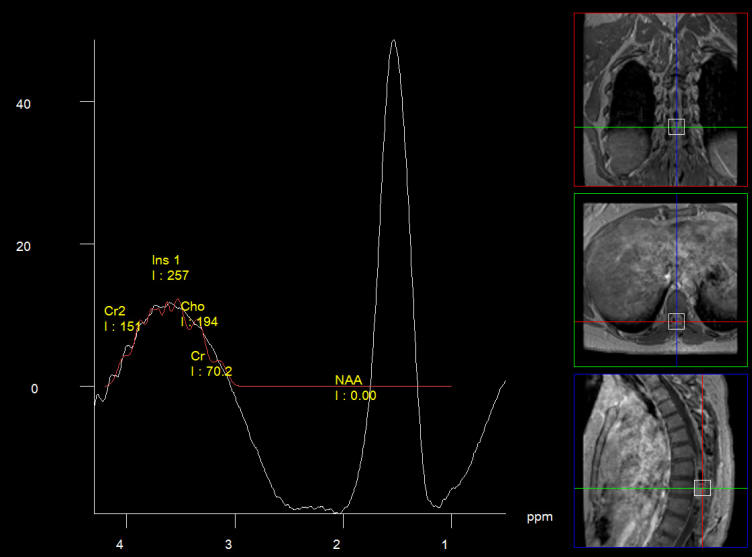
MRI of the dorsal spine with contrast and
myelography and fibertraking and spectroscopy
showing the recent lesions as seen in the below
pictures with abscess formation.
The patient was admitted urgently and given
Decadron 16 mg I/V 8 h. The patient the next
day, showed some movement of both legs, better
of the left, for what it is was decided to
operate her.
The old incision refreshed and the partially
laminectomized D6 was completed to regain normal
anatomy. The dura was opened and downward
dissection and meylolysis was performed in the
midline. The lyodura was seen and included in
the incision in the midline. There was another
layer under the lyodura, which was a reactionary
layer to the lyodura, which was also bisected to
obtain maximum release of the spinal cord.
According to MRI data aspiration of the upper
abscess was succeeded and a thick yellow fluid
was obtained. About 3-4 mm sharp incision in the
midline was performed to expose the abscess
cavity, which was irrigated by saline and part
of the capsule with the fluid were sent for
through investigations. There is no CSF coming
nor from the proximal. nor the lower field of
the wound. Intraoperative MRI was done with
contrast was done showing the shrinkage of the
upper major cavity. The left sided dark colored
lesion below the cavity was studied and it was
bony hard and it was drilled away until the
healthy dura was seen medially. The right lower
cavity was aspirated and clear fluid came out
and a small incision around 2 mm was performed
over it to promote escape of any hidden fluid.
The scar was stitched by nylon water-tightly in
such way, that further decompression of the
spinal cord was achieved. Routine closure of the
wound.
Smooth postoperative recovery. The patient
immediately after the surgery could feel her
left leg and some movement of the feet, better
in the left and can with difficulty move the
adductors and abductors of the hips.
Comments
It was decided before surgery, that if
the patient will not improve with Decadron, to abandon the
surgery, but she showed some improvement, for what surgery
was performed to give the spinal cord the best environment
for better healing.
Lyodura inserted in the first surgery
generated another layer inside adherent to the pathologic
spinal cord.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
Inomed MER system
MRI showing the new flare with abscess malformation and the old one
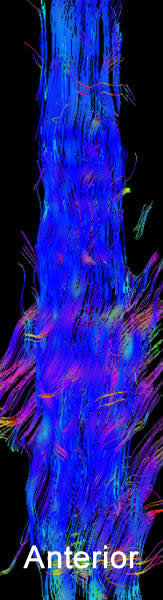
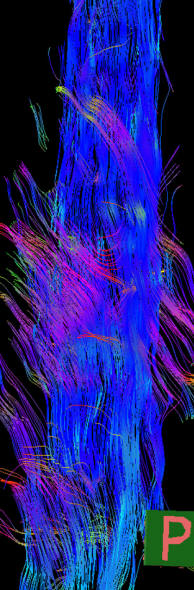
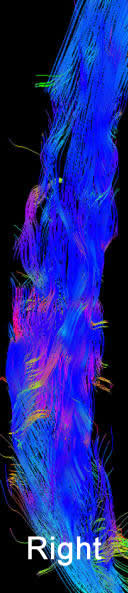
Fibertraking of the spinal cord at the lesion showing some scanty
fibers ready for attack from behind (The middle picture)
Spectroscopy confirming the tbc abscess nature of the flare. High
lipid and the choline is due to contamination of the voxel.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .