Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
16-APRIL-2016 DINA SHAREEF RASHEED 62
YEARS POST KNEE INJURY DROP LEFT FOOT DUE TO DIRECT INJURY TO
THE PERONEAL NERVE.
Anamnesis
The patient was operated by me
16-July-2015 for extruded disc C6-7
and was doing well. The patient then came
27-December-2015 telling that she suffered
falling down 15-October-2015 with fracture of
the left knee and drop left foot. She was
treated at that time with orthopedic surgeons
with Steinmann pin fixation and she came with
orthosis.
On examination: the patient has complete drop
left foot with anaesthesia of the mideodorsal
aspect of the foot excluding the 5th toe. Weak
eversion of the foot.
The patient was sent for investigations: ECS
performed 28-December-2015 confirmed complete
non function of the common peroneal nerve. MRI
of the knee showed severe scar with involvement
of the common peroneal nerve with high grade
injury to the ACL.
The patient then came 10-April-2016 without any
noticeable changes.
Projectional incision over
the course of the left common peroneal nerve and
its divisions with respect to achieve also
fibular collateral ligament exploration. The
common peroneal nerve was exposed proximally.
There is massive scar, that it was very
difficult to follow the nerve down. Exploration
of the common peroneal nerve at the site where
it wind the fibula failed to find it. The septum
between the tibialis anterior and peronius
longus muscle could reveal the deep branch of
the peroneal nerve. All the time it was possible
to achieve peroneal response when using bipolar
stimulation using MultiGen with 4-5 V. Trying to
use ISIS for CNAP protocol failed due to
technical limitations of the machine. The
exposed deep peroneal nerve was followed
proximally and it was possible to see the
superficial division. The neurolysis was
continued up and distally down until the nerve
was seen without interruption from the upper
most of the wound down to its divisions,
The superficial branch was responding to 5-6 V
and the deep branch was responding to 9-10 V.
The divisions were looking healthy without
interruption with fibrillary structure of both
nerves. It was decided to keep the nerves at the
stage of neurolysis. The lateral collateral
ligament was aided with several stitches to
correct the loosening of the the flail lateral
part of the joint and the avulsed bone was
included with this tightening. Routine closure
of the wound.
Smooth postoperative recovery.
She was sent to the ward.
Comments
During the first stages of the procedure
due to massive scar the traditional exposure of the nerve
failed. It was necessary to go far up and down to keep the
integrity of the neural structures.
For more information about CNAP please
click here! It
seems that the setup of ISIS is not intended to perform such
an investigation.
MultiGen was of great help in decision
making. It was possible to see that the superficial branch
was functioning around 30% and the deep branch for 5 %
without obtaining the CNAP, which failed to be obtained
using ISIS Inomed IOM.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Inomed Riechert-Mundinger System, with three point
fixation is the most accurate system in the market. The microdrive and
its sensor gives feed back about the localization.
Inomed MER system
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
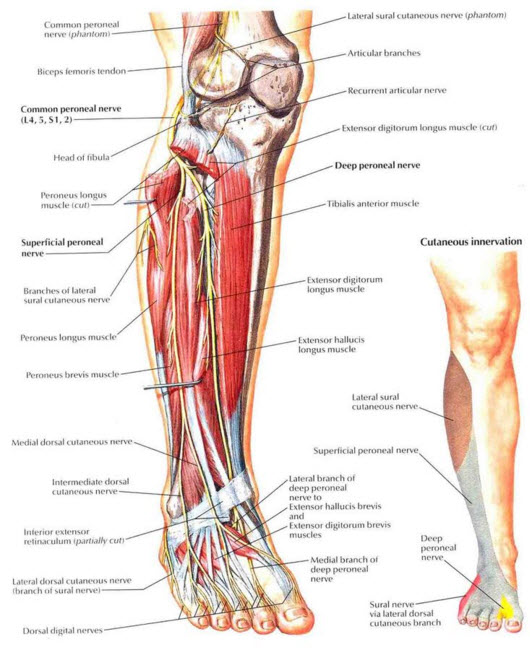
Schematic drawing showing the distribution of the common fibular
nerve, its divisions and sensory areas responsible for each
branch.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .